INTRODUCTION
The proportion of people aged 65 years and over in South Korea is expected to increase from 7.3 % in 2000 to 15.1% in 2020. Accordingly, the health problems of the elderly gain increasing importance in socio-economic terms.1) Dementia is a socially important disease among the senile disorders because it has a high prevalence and deteriorates comprehensive cognitive functions, behaviors and mental functions, considerably inconveniencing vocational and social activities and significantly reducing the quality of life. As the geriatric population increases rapidly, the number of elderly people with dementia is also expected to increase dramatically. In Korea, the incidence of dementia in 2008 was 8.68%, and the number of patients with dementia was estimated at 430,000. It is expected that the prevalence of dementia will increase continuously to an estimated 1,140,000 patients in 2030, with a two-fold increase per 20 years.2) Hence, it is important to attempt to decrease the occurrence of dementia by determining and eliminating its risk factors as well as detecting and treating dementia early.
Many studies have reported relationships between dementia and vascular risk factors such as glucose intolerance, insulin resistance, central obesity, lipid abnormalities and hypertension.3) Hypertension,4,5) diabetes6,7) and hyperlipidemia8,9) play important roles in the pathogenesis of impaired cognitive function and are related to the increase of Alzheimer's disease as well as other types of dementia.10) Metabolic syndrome is a cluster of cardiovascular risk factors, and its prevalence is increasing significantly in Korea. Although diagnostic criteria differ, metabolic syndrome is found in 32.6% of adults 30 years old or older according to the 2005 National Health and Nutrition Survey,11) and a study on diabetes found the prevalence of metabolic syndrome to be 62.0%.12)
With the drastic increase in the prevalence of metabolic syndrome around the world and in South Korea, studies are examining the relationship between metabolic syndrome and cognitive function. Yaffe et al.13) reported a decrease in cognitive function with metabolic syndrome. However, previous studies are limited in that they have not measured cognitive function comprehensively. Most of previous studies have applied simple tests, such as the Mini-Mental State Examination (MMSE), to the evaluation of cognitive function and have not accurately assessed early dementia or mild cognitive disorder.14,15) The MMSE is a simple method that is high in sensitivity and specificity, but it is limited in measuring cognitive function comprehensively. Therefore, it is recommended that cognitive tests for the elderly jointly use the comprehensive measurement tool.16,17) In South Korea, Moon et al.18) reported the relationship between metabolic syndrome and cognitive function in adults older than 50, but no study has examined this relationship among the elderly, who are in the high-risk of dementia and metabolic syndrome.
This study investigated the relationship between metabolic syndrome and cognitive function among elderly persons using the CERA D-K, a more precise evaluation method than MMSE.
METHODS
1. Subjects
The subjects were elderly people who had no difficulties in daily life and consented to participate in the study after receiving a sufficient explanation of its purposes and content. Participants included adults 60 years old and older who were screened at the health promotion center of a university hospital or who attended a health program at the Dongtan public health center from March 2010 through July 2010 in Gyeonggi-do province. Ninety five volunteers were recruited, and 2 were excluded due to cerebrovascular history. Thus, cognitive function tests were performed on 93 subjects. When a subject visited the hospital, an inquiry and history taking were conducted, which included information on age, gender, education, vocation, smoking, drinking, exercise and underlying disorders and cognitive functions; and a cognitive function test was performed. Smokers were classified into current smokers, past smokers who had not smoked in the past year, and non-smokers who had never smoked. Drinking frequency was divided into no drinking, drinking 6 or more times per week, 3-5 times per week, 1 or 2 times per week and less than once per week. Frequency of exercise for 30 minutes or more was categorized into 3 or more times a week, once or twice a week and hardly ever. Trained nurses measured participants' height, weight, waist circumference and blood pressure and conducted blood tests. Excluded from the study are those who had or were suspected of having dementia (based on the DSM-IV), had any problems in daily life, were unable to communicate or had cerebrovascular disease or cancer that might lower cognitive function.
2. Evaluation of Cognitive Function
Experienced doctors evaluated the subjects using the Korean version of the Consortium to Establish a Registry for Alzheimer's Disease (CERAD-K).19) The CERAD-K neuropsychological assessment battery (CERA D-K[N]) is a standardized evaluation tool for the early diagnosis of dementia. The test takes a short time, approximately 30-40 minutes, and is relatively easy to perform. Thus, it is very useful for the evaluation of elderly patients with dementia. The CERAD-K neuropsychological evaluation consists of nine neuropsychological subtests (verbal fluency test, modified Boston naming test, Korean version of the mini-mental state examination [MMSE], word list memory, vonstruction praxis, word list delayed recall, word list recognition, construction recall, and trail making tests A and B). The total CERA D-K score was calculated by adding the scores on six tests: the verbal fluency test, modified Boston naming test, word list memory, construction praxis, word list delayed recall, and word list recognition. The maximum of total CERA D-K score was 100 points.20,21)
Depression was evaluated using the Short Geriatric Depression Scale, Korean version (SGDS-K). The SGDS-K consists of 15 questions and has been shown to be a reliable and valid screening test for geriatric depression.22) The optimal SGDS-K cutoff point for depression was defined as 8 points.
3. Metabolic Syndrome
Meeting the following 3 items or more was defined as metabolic syndrome on the basis of National Cholesterol Education Program's Adult Treatment Panel III (NCEP-ATP III).23) Abdominal obesity was defined as the waist circumference of ≥ 90 cm (male) and ≥ 85 cm (female), which were recommended by the Korean Society for the Study of Obesity (KSSO)24) in 2005: 1) waist circumference (WC) ≥ 90 cm for men or ≥ 85 cm for women; 2) TG levels ≥ 150 mg/dL; 3) HDL levels < 40 mg/dL for men or < 50 mg/dL for women; 4) systolic blood pressure (SBP) ≥ 130 mm Hg or diastolic (DBP) ≥ 85 mm Hg, or the use of antihypertensive medication; and 5) fasting plasma glucose (FBS) ≥ 100 mg/dL, or the use of anti-diabetic medication or insulin.
4. Statistical Analyses
The data were analyzed using the SPSS ver. 13 (SPSS Inc., Chicago, IL, USA). The results are expressed as the mean ± SD. Chi-square test and independent samples test were used to investigate socio-demographic characteristics and biochemical tests according to metabolic syndrome. Each item of the CERAD-K test was assessed according to metabolic syndrome with a multivariate covariance analysis (MANCOVA) after adjustment for age, education, and alcohol consumption. A multiple regression analysis was conducted to determine cognitive function's association with age, gender, education, smoking, alcohol drinking, exercise, depression and metabolic syndrome. P-values of less than 0.05 were regarded as statistically significant.
RESULTS
1. Comparison of the General Characteristics and Biochemical Tests according to Metabolic Syndrome
Of the 93 subjects, 48 subjects (24 male, 21 female) had metabolic syndrome. The incidence was higher in female subjects than male (63.8% vs. 31.4%). Of the 48 subjects with metabolic syndrome, 20 (41.6%), 14 (29.1%), and 4 (8.3%) were taking anti-hypertensive drugs, lipid-lowering agents and oral hypoglycemic agents, respectively. There was no significant difference in age, education, smoking, drinking, exercise or depression between the group with metabolic syndrome and the control group, but women made up a significantly higher part of the group with metabolic syndrome. Compared to the control group, the group with metabolic syndrome showed a significantly higher average in body mass index, blood pressure, waist circumference and lipid concentration (Table 1).
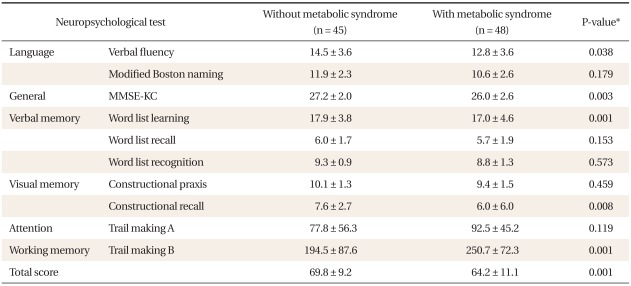
2. Performance on the Cognitive Function Test according to the Presence of Metabolic Syndrome
The total CERA D-K score was 64.2 ± 11.1 in the group with metabolic syndrome, which was significantly lower compared to the value of 69.8 ± 9.2 in the control group. In the comparison of CERA D-K items, significantly lower scores were observed in the Verbal Fluency test, the Construction Recall test, the Word List Learning test, and Trail Making B in the group with metabolic syndrome. The MMSE-KC score was 26.0 ± 2.6 in the group with metabolic syndrome, which was significantly lower compared to 27.2 ± 2.0 in the control group (Table 2).
3. Relationships between Metabolic Syndrome and Cognitive Function
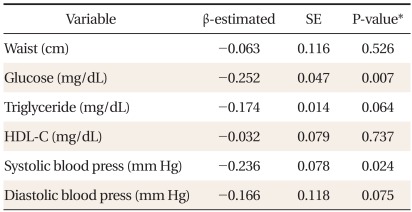
A regression analysis was conducted on age, gender, education, physical activity, smoking, drinking, depression and metabolic syndrome (Table 3). The presence of metabolic syndrome, alcohol consumption, and education were significantly associated with the total CERA D-K score (P < 0.05). However, the SGDS-K score had no association with the total CERA D-K score. In terms of education level, cognitive function scores were significantly higher among people with more than 7 years of education compared to those with 3 years or less. In a multiple regression analysis using metabolic risk factors (waist circumference, TG, HDL, blood pressure, FBS), glucose and systolic blood pressure levels affected the total CERA D-K score (R2 = 29.4%, P < 0.05) (Table 4).
DISCUSSION
In this study, the prevalence of metabolic syndrome was 63.8% in women, which was significantly high compared to the prevalence in men (31.4%). This figure is close to the findings of a previous study of the total population (63.4% female, 34.1% male).11) The cognitive function was significantly high in participants with 7 or more years of higher education compared to those with 3 or fewer years of education. This finding supports the hypothesis that a higher education level delays the occurrence of dementia by supplementing cognition.25) The cognitive function was significantly high in the drinking group compared to the non-drinking group. This finding is in contrast to the findings from previous studies that drinking increased the risk of dementia.26) In terms of drinking frequency, 93.1% of participants drank less twice. According to previous studies, a small amount of alcohol (i.e., 1-3 standard drinks or less a day) prevents the reduction of cognitive function, reduces the risk of dementia27) and deters the progress of dementia in patients with mild cognitive disorder.28) However, the present study is limited by not determining accurate amount and types of alcohol drinking. It seems necessary to analyze this relationship to cognitive function based on an accurate drinking history. Depression symptoms were serious in the Alzheimer-type dementia group compared to the control group.29) Many studies report that depression is closely related to the lowering of cognitive function, but this study found no relationship between SGDS-K scores and cognitive function. Because the subjects had normal cognitive function with an MMSE score over 26 points and an SGDS-K score under 8 points, it seems that no depression symptoms were observed with regard to the changes in cognitive function. However, it will be necessary to conduct additional studies on elderly people in the future.
Recently, many studies have reported a relationship between metabolic syndrome and cognitive function. According to a prospective study of adults aged 70 years or older, cognitive function declined significantly in the group with metabolic syndrome.13) In a 3.5-year prospective study of 2,097 patients 65 years or older with mild cognitive disorder, Solfrizzi et al.30) reported a significant increase in the risk of progressing from mild cognitive disorder to dementia when accompanied by metabolic syndrome. Additionally, it is suggested that dementia increases with the increase in vascular risk factors, such as hypertension, diabetes, hyperlipidemia and smoking, in middle age.31) Based on the mixture of cardiovascular risk factors, metabolic syndrome seems to be related to cognitive function. In South Korea, Moon et al.18) reported that cognitive function decreased in adults with metabolic syndrome. However, the authors assessed cognitive function with the MMSE-K and did not perform a comprehensive and detailed analysis of cognitive function. In addition, depression symptoms were not considered. We assessed the relationship between metabolic syndrome and cognitive function in elderly Korean people using the CERAD tool. In this study, CERA D-K total scores were 64.2 ± 11.1 in the metabolic syndrome group and 69.8 ± 9.2 in the control group, which is consistent with previous findings on the total CERA D-K score in the Korean population.21) Cognitive function decreased in the metabolic syndrome group compared to the normal control group, especially on the verbal fluency test, construction recall test, word list learning test, trail making B, and the total CERAD-K score. This result might indicate the reduction of frontal lobe functions related to initial changes in dementia.
In this study, the presence of metabolic syndrome was significantly associated with cognitive function. Among the metabolic risk factors, fasting plasma glucose and triglyceride levels affected the CERAD-K total score. Many studies have examined the mechanism by which metabolic syndrome affects cognitive function. Insulin resistance and hyperinsulimenia in metabolic syndrome cause a decrease in glucose use and energy metabolism in the cerebral cortex than in other tissues.32) Furthermore, in cases of hyperinsulimenia, insulysin, which decomposes the beta amyloid and plays an important role in Alzheimer's dementia, is better combined with insulin, thus depositing beta amyloids and increasing the phosphorylation of tau proteins.33) Cholesterol, a main component of myelin and cell membrane, plays an important role in maintaining the functions of cerebral tissues. According to Eckert et al.,34) there is a decrease in the membrane fluidity of the hippocampus as a memory center in Alzheimer's dementia, which may be related to cholesterol disorder. Beta amyloids destroy the cell membrane structure of cerebral tissue. A low cholesterol concentration causes a reduction in beta amyloid formation in hippocampus neurons, thus delaying the occurrence of Alzheimer's dementia.34) Hypertriglyceridemia changes cerebral blood by increasing the viscosity of blood and lowers cognitive function by causing arteriosclerosis.35) Hypertension is said to decrease the number of nicotinic receptors sensitive to acetylcholine and to cause cerebrovascular diseases, cerebral infarction and cerebral gray substances, arteriosclerosis and lower cognitive function.36) A chronic high blood sugar level deters the synthesis and secretion of cerebral acetylcholine37) and causes the loss of neurons in the cerebral cortex and the reduction of glucose levels in cells, leading to a decrease in cognitive function.38)
Given the studies that suggest the high possibility that a decrease in cognitive function or mild cognitive function disorder will develop into dementia,39) elderly individuals with metabolic syndrome have a lower cognitive function compared to the control group, and they are likely to develop dementia, although they do not currently suffer from dementia. Accordingly, the early detection and correction of metabolic syndrome in adults is likely to decrease cardiovascular diseases and to reduce the decrease of cognitive function and the risk of dementia. Given that early detection and treatment are effective for senile dementia, it seems that the precise assessment of cognitive function will be helpful for metabolic syndrome patients.
Our study has the following limitations. First, the subjects of this study are individuals who participated in a health promotion program of a hospital. Thus it is necessary to be cautious in applying the study results to normal population groups. Second, there were more women in the group with metabolic syndrome than in the control group. However, this trend is similar to the gender distribution in the elderly Korean population. There were statistically significant relationships between metabolic syndrome and cognitive function even after adjusting for gender and education. Third, this was cross-sectional study to assess the relationship between metabolic syndrome and cognitive function, but it was difficult to evaluate causal relationships. However, this study is significant in that it analyzed the relationships between metabolic syndrome and cognitive function in elderly Korean individuals using the CERA D tool. It will be necessary to perform a prospective study to determine whether metabolic syndrome causes cognitive dysfunction or dementia and whether the correction of cardiovascular risk factors can improve cognitive function.