INTRODUCTION
Osteoporosis is a common disorder characterized by reduced mineral density and bone mass, microarchitectural deterioration and increased skeletal fragility, and it results in an increased risk of fracture.1) Osteoporosis occurs in both males and females but is particularly common among women following menopause when bone turnover increases and the rate of bone resorption exceeds that of bone formation. Corresponding with an aging society, the public health impact of osteoporosis is enormous, affecting 200 million individuals worldwide. The reported prevalence of osteoporosis in Caucasian women older than 50 years of age varies from 7.9% to 22.6%.2,3) In a community-based cohort study consisting of 1,547 men and 1991 women in Korea, the crude prevalence of osteoporosis in subjects aged 40 to 79 years was 13.1% for men and 24.3% for women based on World Health Organization (WHO) criteria.4)
The goal of osteoporosis treatment is to reduce the fracture risk by preventing further loss of bone mineral density (BMD). Bisphosphonate inhibits bone resorption by reducing osteoclast number and function, and alendronate is one of the most potent and widely used bisphosphonates. In many European countries and in the United States, alendronate is being used clinically for the treatment of osteoporosis because of its established effects on bone density and fracture prevention.5,6) The recommended dose of alendronate is generally 10 mg daily or 70 mg weekly. Continuous treatment with 10 mg of alendronate daily for 10 years is associated with sustained therapeutic effects on bone density and remodeling.7) Studies in Japan found that 5 mg/d of alendronate increased BMD in Asian postmenopausal women with osteoporosis to a level similar to that achieved with 10 mg/d in Caucasian women.8,9)
Vitamin D enhances intestinal absorption of calcium and thereby affects bone mineralization. Low levels of vitamin D are associated with negative calcium balance, and a compensatory rise in parathyroid hormone, which results in excessive bone resorption. It has been estimated that 1 billion people worldwide could be classified as being vitamin D deficient or insufficient.10) Postmenopausal Korean women are at an increased risk of low vitamin D levels due to lack of exposure to sunshine, genetic traits, air pollution, and dietary habits.11) Several studies have demonstrated the positive effects of combining the use of active vitamin D (i.e., calcitriol) with antiresorptive agents such as calcitonin and bisphosphonates.12,13) Those results have led to the development of drugs such as Maxmarvil, which contains a combination of 5 mg alendronate and 0.5 ┬Ąg calcitriol.
The present study evaluated the efficacy and safety of Maxmarvil in Korean postmenopausal women with osteoporosis. We examined the effect of Maxmarvil on BMD, and identified factors associated with improved BMD.
METHODS
1. Study Participants
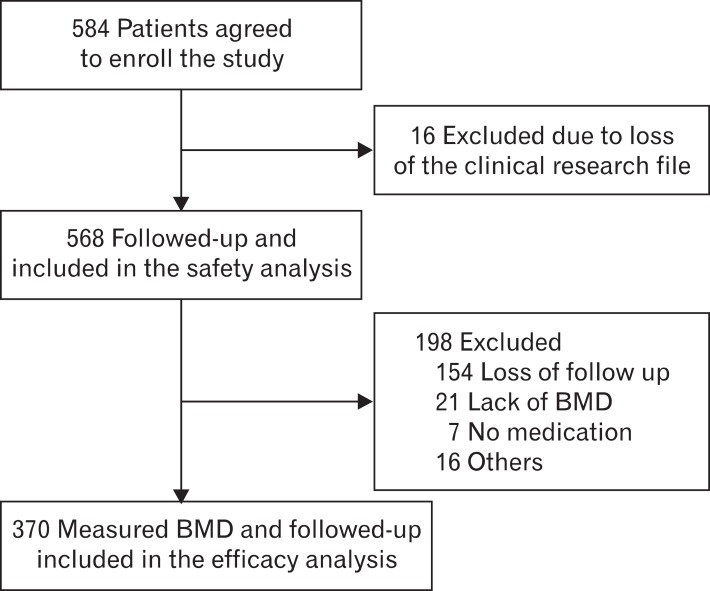
The study recruited postmenopausal women who visited family physicians in 12 hospitals for osteoporosis or osteopenia treatment between September 2007 and August 2010. This study was approved by the institutional review board of the Asan Medical Center (2007-0400). Patients were excluded if they had a history of Maxmarvil treatment, a history of serious medical problems, or secondary osteoporosis related to systemic glucocorticoid therapy. The study comprised a safety analysis and an efficacy analysis. The safety analysis involved the initially enrolled 568 patients who had at least one follow-up visit after taking Maxmarvil. In the efficacy analysis, 198 patients were excluded because they were lost at follow-up (154 patients), there were missing values (21 patients), they refused to take medication (7 patients) or they discontinued treatment due to adverse events (16 patients). Therefore, 370 of the original 568 patients were involved in the efficacy analysis (Figure 1).
2. Self-administered Questionnaire
Demographic characteristics including marital, educational, and income status were assessed using a self-questionnaire at the first visit. Information regarding known health risks such as smoking, heavy drinking, exercise habits, and current medication use were also obtained. Patients were classified as current smoker, ex-smoker, and never a smoker, and as non-drinker or drinker. Exercise habits were categorized as less than once per week, one to two times per week, and three or more times per week.
3. Calcium Intake Measurement
A simple semi-quantitative food frequency questionnaire (SQFFQ) was used to assess the calcium intake of the patients. The questionnaire included questions regarding the dietary intake of 30 food items that contain calcium. Eight categories were used to determine intake frequency: hardly ever, once a month, two or three times a month, two or three times a week, four to six times a week, daily and over twice daily. Daily calcium intake and calcium ingestion rate based on food groups were calculated using the questionnaire data. The questionnaire was found to have validity when compared to previous semi-quantitative calcium intake frequency questionnaires (Pearson correlation coefficient, 0.50; Spearman correlation coefficient, 0.49). The prediction equation for estimating daily calcium intake from the SQFFQ was (daily calcium intake) = 14.928 ├Ś (calcium intake from SQFFQ)0.527.14)
4. Drug Usage
Study subjects were given Maxmarvil (5 mg alendronate and 0.5 ┬Ąg calcitriol) daily for 1 year, after which they were evaluated. Patients were directed to take Maxmarvil in the early morning before breakfast with sufficient water, and were instructed to then remain upright for at least 30 minutes. Adverse events associated with the drugs were assessed at 3, 6, 9, and 12 months.
5. Bone Mineral Density Measurement and Efficacy Evaluation
Lumbar spine BMD was measured using dual energy X-ray absorptiometry (DEXA). The BMD of the lumbar spine (L2-L4) was measured at commencement and after 12 months of treatment. A statistically significant increase in BMD was defined as a change exceeding the least significant change (LSC).
Calculation of the LSC requires consideration of the confidence interval. Specifically, if the LSC is determined at 95% confidence, the precision error (PE) is multiplied by 2.77 (LSC = 2.77 ├Ś PE).15) The PEs for each hospital's DEXA ranged from 0.7% to 1.5%. Therefore, we obtained the LSC from the median precision errors of each hospital's DEXA, and BMD changes that exceeded the LSC were considered to be significant. Using WHO criteria, osteoporosis was defined as a bone mineral density 2.5 standard deviations or more below the mean peak bone mass measured using DEXA.
6. Statistical Analyses
The average BMD differences before and after treatment were compared using paired t-tests. Chi-square and Fisher's exact tests were used in univariate analyses to identify factors associated with BMD improvement. Logistic regression was used for multivariate analyses. The level of statistical significance was set at 0.05, and IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA) was used for all statistical analyses. Data are expressed as mean, standard deviation, and odds ratio.
RESULTS
1. Baseline Clinical Characteristics
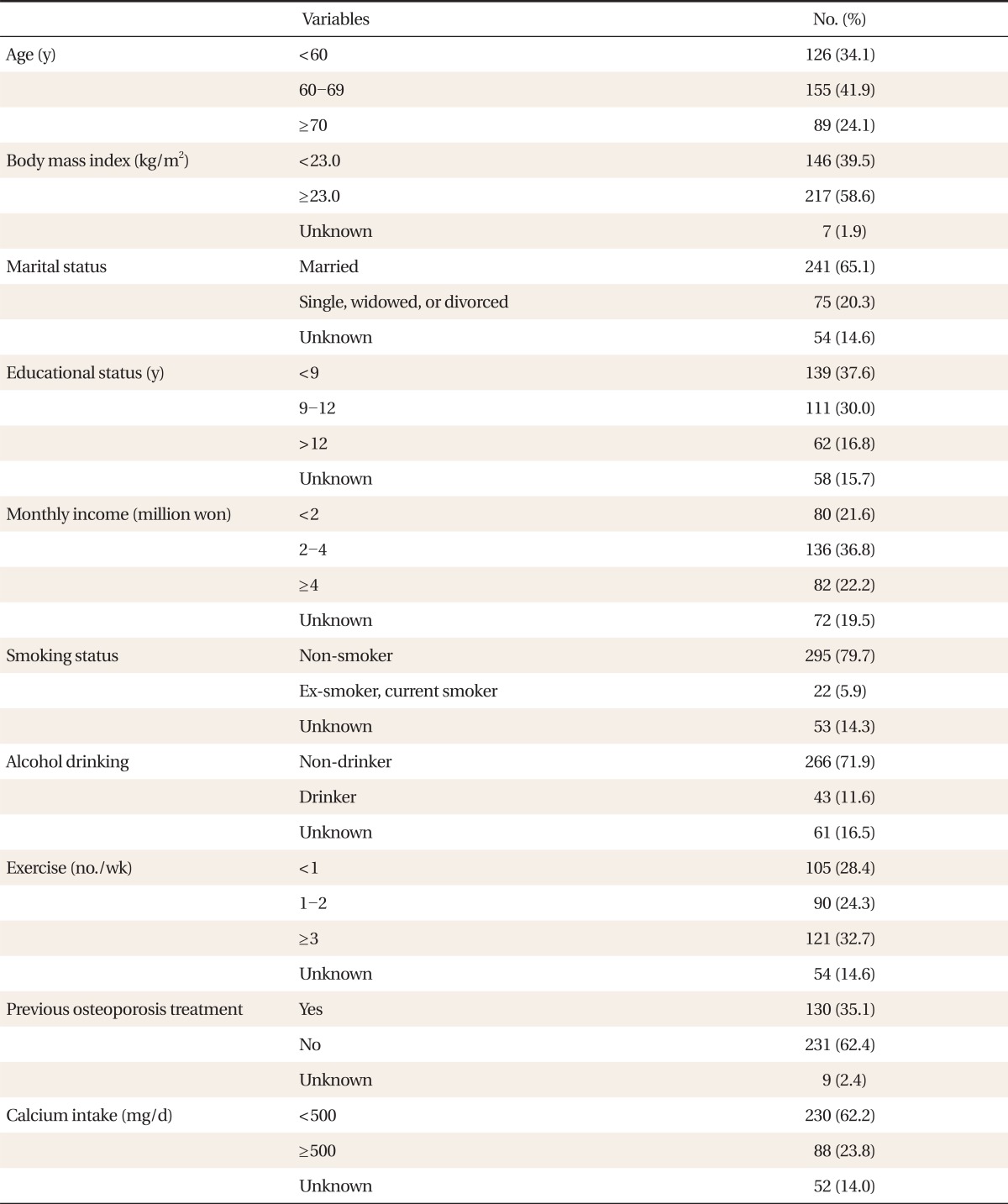
The average patient age was 63.4 ┬▒ 8.9 years and average body mass index (BMI) was 23.6 ┬▒ 3.1 kg/m2. Most patients had never smoked and were non-drinkers. In terms of physical activity, 28.4% partook less than once per week and 32.7% partook 3 or more times per week. Nearly one third (35.1%) had previously been treated for osteoporosis. Based on the SQFFQ responses, no patients had a daily calcium intake Ōēź 1,500 mg, which is the recommended dietary allowance (RDA) for women. There were 230 (62.2%) patients who had a daily calcium intake of < 500 mg (Table 1).
2. Changes in BMD
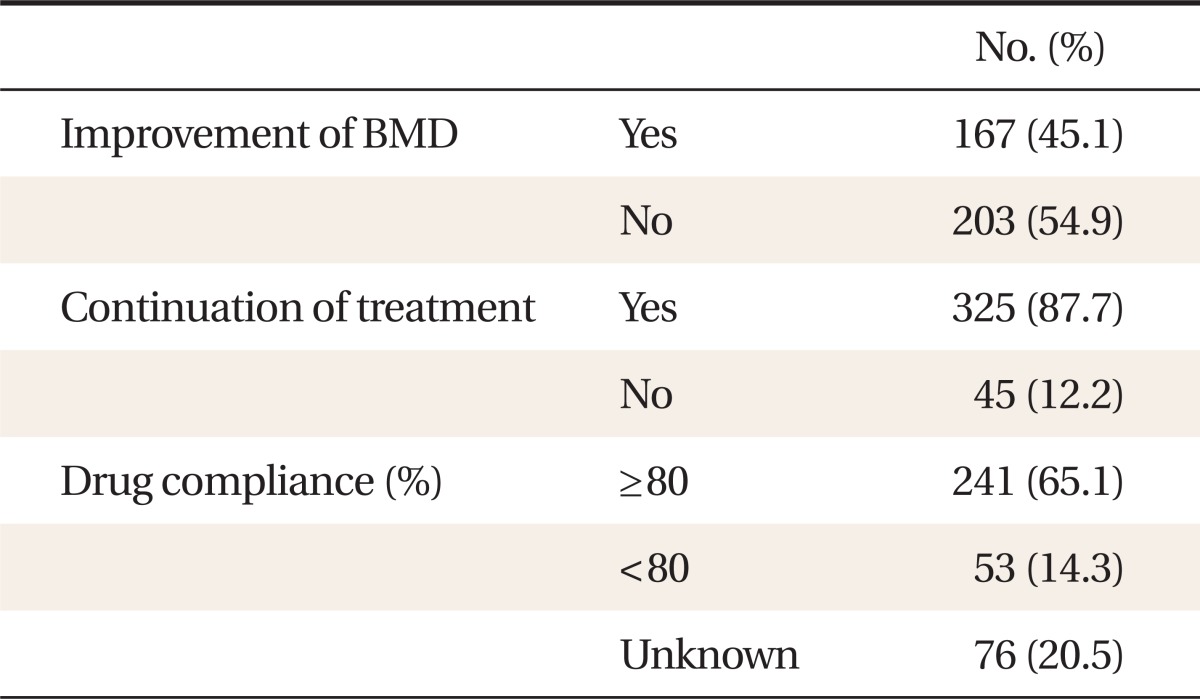
The pre-treatment average lumbar BMD was 0.81 ┬▒ 0.12 g/cm2, and the post-treatment average was 0.84 ┬▒ 0.13 g/cm2. The average improvement in lumbar BMD was 3.4% ┬▒ 6.4% (P < 0.001) (Figure 2). Of the 370 subjects who were included in the efficacy analyses, 167 (45.1%) showed improvement in lumbar BMD. Three hundred and twenty-five 325 (87.7%) patients continued the treatment after 1 year and 65.1% showed good compliance (i.e., >80% compliance) (Table 2).
3. Factors Associated with BMD Improvement
Univariate analysis showed that continuation of treatment and good compliance (i.e., >80% compliance) were associated with BMD improvement (P < 0.05) (Table 3). Age, BMI, marital status, monthly income, educational status, smoking, alcohol, exercise, and calcium intake showed no significant association.
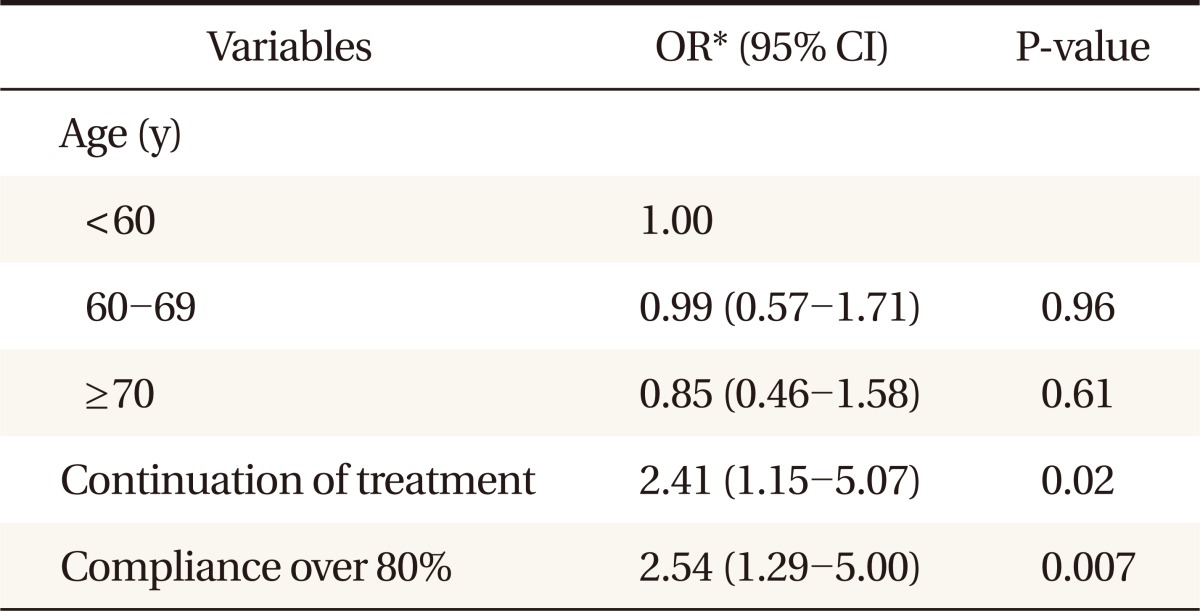
Multiple logistic regression analysis was performed to evaluate the independent factors associated with improved bone mineral density. The factors which were associated with bone density in univariate analysis and age were included in the analysis. Thus, multivariate logistic regression was performed including age, continuation of treatment, and compliance over 80%. According to the analysis, treatment continuation and good compliance (>80%) were associated with improvement of BMD (Table 4).
4. Adverse Events
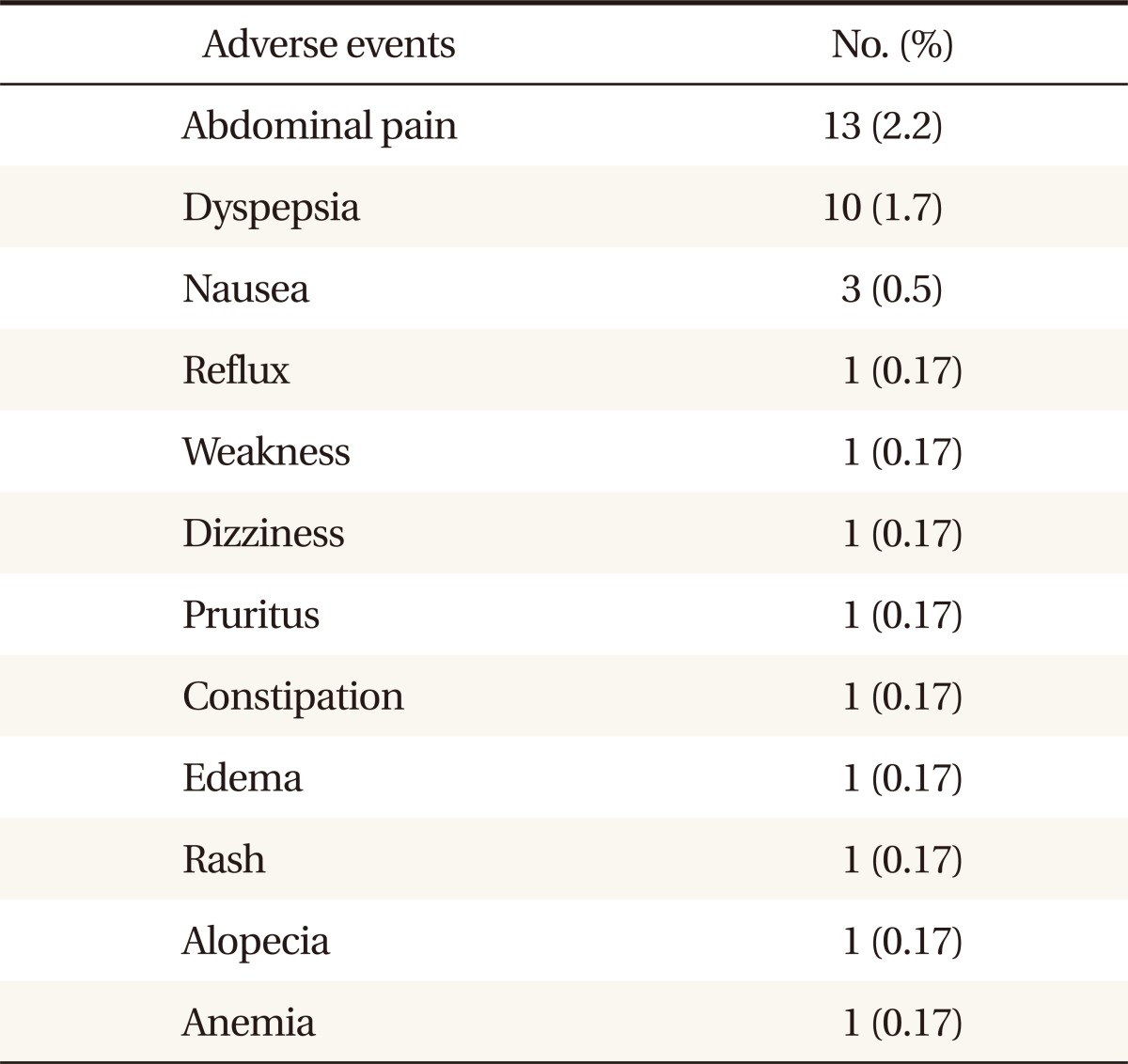
Safety analyses involved 568 patients. A total of 35 adverse events were reported in 32 subjects (5.6%). The most common adverse event was abdominal pain, which occurred in 13 patients (2.2%), followed by dyspepsia (1.7%) and nausea (0.5%). In addition, there was one case each of dizziness, weakness, pruritus, constipation, and edema (Table 5). Sixteen patients (2.8%) discontinued treatment as a direct result of adverse events. There were no serious adverse events leading to cessation of drug treatment.
DISCUSSION
The present study found that daily treatment with Maxmarvil for 12 months resulted in an increase in lumbar BMD. Considering the LSC for each hospital, we found that 167 subjects (45.1%) showed BMD improvement. Factors associated with BMD improvement were good compliance and continuation of treatment.
In the current study, the average improvement in lumbar BMD was 3.4% ┬▒ 6.4%. Another study conducted in Korea also using Maxmarvil reported a BMD increase of 2.42% ┬▒ 0.5% after 24 weeks of treatment.16) It is interesting that that amount of improvement was somewhat similar given that the treatment period was about half the duration of that in the present study. In a randomized open study including 226 postmenopausal women with osteoporosis, 10 mg alendronate plus 0.5 ┬Ąg alfacalcidol for 12 months was found to increase BMD by 4.3%.
The generally recommended dosage of alendronate is 10 mg daily or 70 mg weekly. However, previous studies conducted in Japan showed that 5 mg/d of aldendronate for 3 years was also effective in increasing BMD and reduced the risk of vertebral fractures.8) In addition, another study reported that 2.5 mg/d of alendronate had a positive effect on BMD, and that the effect was not significantly different from a 10 mg/d dosage.17) Compared with Caucasians, Asians have smaller body size and a lower dietary intake of calcium, therefore the recommended drug dosage established for Caucasians may not be appropriate for Asians.17)
Vitamin D deficiency is now a worldwide problem even in developed countries. In Korea, the prevalence of 25(OH) D levels less than 50 nmol/L during the wintertime is reported to be 90.1%.18) Furthermore, calcium intake for most Koreans is below the RDA. In the present study, no patients had a daily calcium intake >1,500 mg, which is the RDA for postmenopausal women. The superiority of calcitriol compared to native vitamin D in preventing bone loss and fractures has been established. In addition, combined treatment with alendronate and vitamin D analogs seems to be more effective, as compared to the respective monotherapies.19)
In the present study, multivariate analysis, which adjusted for age and other factors, found that continuation of treatment and good compliance were associated with BMD improvement. Drug compliance and adherence are important factors in successful treatment. In a previous study of postmarketing surveillance for the efficacy and safety of residronate, good compliance was associated with BMD improvement.20) And studies assessing the consequences of poor compliance and persistence in patients who did not follow their dosing regimens demonstrated lower BMD gains and increased risk of fracture.21,22) Dosing frequency is one of the factors contributing to poor adherence, and despite the daily regimen of Maxmarvil, the compliance and persistence in our study was high (65% and 87.7%, respectively). This may reflect the use of a combined drug, as against having to take bisphosphonate and calcitriol separately.
The present study used the simple SQFFQ to obtain calcium intake information. Using 500 mg/d of calcium as a referent, patients with an intake of Ōēź500 mg/d had an odds ratio for BMD improvement of 0.68 (95% confidence interval, 0.41 to 1.13). No association was observed between calcium intake and BMD improvement, either before or after adjustment. BMD improvement from calcium intake was expected to be relatively small because the efficacy of Maxmarvil was great. However, recall bias cannot be completely excluded because the measurement method used was a self-reporting questionnaire.
Drug safety is a critical issue. The overall adverse event rate in this study was 5.6%. Abdominal pain and dyspepsia were the most common adverse events, and accounted for more than half of the total events. The types of adverse events in this study did not differ from those reported in other bisphosphonate studies.23,24) The proportion of patients who experienced adverse events that led to discontinuation was 2.8% (16 patients). Therefore, Maxmarvil was found to be well tolerated with no serious adverse events and showed a low dropout rate during the study period.
The significance of this study is that it was a multicenter study conducted at 12 medical centers targeting people from various regions, which differentiates it from other studies. In addition, unlike other studies, this was an outpatient-oriented survey in a primary care setting, so the findings can be broadly applied with greater confidence. The study showed Maxmarvil had long-term efficacy up to 1 year, and it was possible to assess an accurate drug response due to the high drug compliance. Since all the centers measured BMD with DEXA, a standardized efficacy assessment was feasible.
The present study had several limitations. First of all, as our study analysis included the subjects who followed the study protocol completely, the efficacy of Maxmarvil could be exaggerated. In addition, this study did not include a placebo-controlled group. We could only specify the result by absolute changes in BMD before and after treatment. Therefore, we could not ascertain the direct relationship between Maxmarvil efficacy and fracture reduction. Although opinions differ as to whether fracture risk reduction is attributable to BMD improvement, major clinical trials have demonstrated that alendronate treatment reduced vertebral and non-vertebral fractures by 48% and 47%, respectively.25,26) Moreover, the relationship between BMD increase and fracture risk reduction is not proportional; a small BMD improvement has been found to cause a remarkable reduction in fracture risk.27,28) Although our study did not include a control group, by considering the absolute changes in BMD after treatment, we can assume that it would have positive effects on fracture reduction.
In conclusion, this survey of postmenopausal women with osteoporosis in a primary care setting found that Maxmarvil was efficacious, safe, and well tolerated.