INTRODUCTION
Smoking is one of the preventable causes of death.1) According to a report on the global tobacco epidemic in 2011 by the World Health Organization, smoking has caused 6 million deaths and economic loss of over a hundred billion won each year worldwide.2)
In the USA, the number of deaths related to smoking reached 443,000 per annum during 2000 to 20043) and some of the research carried out in Korea revealed that smoking was an important inducing factor of diabetes, ischemic heart disease, chronic obstructive pulmonary disease, and stroke, and that the level of contributing risk of smoking toward chronic diseases in males was as high as 30%.4) In spite of the multifaceted efforts to reduce the hazards of smoking, the smoking rate in adults over the age of 19 was still high at 27.2% in the Korean national health and nutrition survey of 2009.5)
Consultation by a doctor on smoking cessation is effective for reducing smoking rates. According to past research in Korea, smoking cessation education carried out at the time of the health check-up and outpatient treatment at a smoking cessation clinic was effective in improving the level of motivation and success rate of smoking cessation.6,7)
However, no studies have been conducted concerning the effect of education on smoking cessation outside the hospital in Korea. Expiratory carbon monoxide (CO) is a measurement which has close correlation with carboxyhemoglobin concentration in the blood, and has been increasingly used for the verification of smoking status because measurement of expiratory CO is convenient and non-invasive, gives results quickly, and is inexpensive.8) This study aimed to examine the effect of smoking cessation education on smoking cessation in adult male office workers using the measurement of expiratory CO values taken outside the hospital.
METHODS
1. Subjects and Methods
From April 1st, 2012 to May 10th, 2012, male smokers over the age of 19 with a smoking history of more than 5 packs of cigarettes were chosen as candidates of this study in the urban streets of Seoul. Among these candidates, those who gave consent after having received a sufficient explanation on the purpose and confidentiality of personal information were selected as subjects.
Subjects were divided into an education group and a control group by a cluster extraction method. They were allocated 10 to 20 subjects each day into the control group then the education group on the following day. One medical doctor wearing a lab coat conducted the survey and allocated the subjects in each group. On the basis of the results of domestic research that the sensitivity and specificity are 88.6% and 97.1%, respectively, when the standard value of CO for the distinction between a smoker and non-smoker is set at 9 ppm by using the Micro III smokerlyzer (Bedfront Scientific Ltd., Rochester, UK),9) those with a value of less than 9 ppm were excluded from the education group. In addition, those subjects in both the education group and control group who had received smoking cessation counseling, a health check-up, or hospitalized treatment during the past year were excluded.
For the cases of the education group, expiratory CO values were measured only for subjects who indicated voluntary consent. CO measurements took approximately 1 minute to acquire. For the education group, the expiratory CO measurement and education on the hazards of CO, more than 4,000 chemical substances and carcinogenic substances absorbed were given. Moreover, a doctor personally explained the health advantages of quitting smoking for about 5 to 10 minutes and distributed information materials on smoking cessation. We used Micro III smokerlyzer (Bedfront Scientific Ltd., Rochester, UK) for the expiratory CO measurements.
The self-help material included a booklet that contained a wide range of information including that on chemical substances and carcinogenic substances in cigarettes, the actual status of death due to smoking, the action and mechanism of nicotine addiction, the affirmative effect of smoking cessation, and the means of overcoming withdrawal symptoms of smoking.
For the control group, a measurement of expiratory CO was not carried out, but subjects were given self-help materials on quitting smoking after having completed the questionnaire.
The questionnaire included questions on socio-demographic characteristics such as age, marital status, monthly household income and educational level, total number of cigarettes smoked, average frequency of drinking alcoholic beverages, number of attempts to quit smoking in the past (for more than 24 hours), level of motivation for quitting smoking, and assessment of nicotine dependence using the Fagerstrom test for nicotine dependence (FTND). The subjects were asked to fill in the questionnaire during a one-on-one encounter on the street.
The level of motivation to quit smoking was categorized on the basis of a transtheoretical model.10) Preparing to quit smoking within 30 days was categorized as preparation stage, considering quitting smoking within 6 months as contemplation stage, and not considering quitting smoking at the moment as precontemplation stage, respectively.
A valid and reliable Korean translated version of the FTND was used,11) and a score of less than 2 points was categorized as very low dependence, a score of 3 to 4 points as low dependence, a score of 5 points as medium dependence, a score of 6 to 7 points as high dependence, and a score of more than 8 points as very high dependence.12)
After 4 weeks, a follow-up questionnaire was conducted via mobile phone or email address to assess the improvement of the level of motivation and whether or not the subject had smoked at anytime in the past 7 days. In the case of the level of motivation to quit smoking, a conversion from the precontemplation stage to the contemplation or preparation stage, or from the contemplation stage to the preparation stage was determined to be an improvement in the level of motivation to quit smoking, and the cases of successful smoking cessation were also included. This study was carried out after having received the approval of the institutional review board of Inje University Seoul Paik Hospital.
2. Statistical Analysis
A chi-square test or Fisher's exact test was conducted to compare the education group and control group for significant differences in marital status, educational level, monthly household income, frequency of alcoholic consumption, number of attempts made in the past to quit smoking, and level of motivation to quit smoking for both groups. An independent sample t-test on age, total number of cigarettes smoked, and FTND were carried out to compare the two groups.
The Fisher's exact test was carried out 4 weeks later to analyze whether smoking cessation education had an effect on success or changes in the level of motivation to quit smoking. In order to find the variables that affected the success and improvement in the level of motivation to quit smoking, a chi-square test or Fisher' s exact test was conducted. Multiple logistic regression analysis was carried out on monthly household income, initial level of motivation to quit smoking, age, educational level, number of attempts made in the past to quit smoking, total number of cigarettes one smoked, and Fagerstrom score that were found to impart an effect on the level of motivation to quit smoking as the result of analysis. SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) was for statistical analysis with a level of significance of less than 0.05.
RESULTS
A total of 108 subjects (51 in the education group and 57 in the control group) participated in the study. The follow-up survey to determine the success or change in the level of motivation to quit smoking was conducted 4 weeks later via mobile phone or e-mail address given by the subjects at the time of initial survey. A final analysis was carried out on a total of 95 subjects (44 in the education group and 51 in the control group) with the exclusion of 12 subjects for whom follow-up survey failed (6 in the education group and 6 in the control group) and 1 subject (education group) who underwent a health check-up during the last 1 year at the time of initial survey and had an expiratory CO value of 6 ppm.
A comparison of the general characteristics of the education group and control group showed no significant difference between both groups in terms of marital status, educational level, monthly household income, average frequency of alcoholic consumption, or number of attempts made in the past to quit smoking for more than 24 hours. However, there were significant differences in age (P = 0.022), total number of cigarettes smoked (P = 0.012), level of motivation to quit smoking (P = 0.032), and Fagerstrom score (P = 0.024) (Table 1).
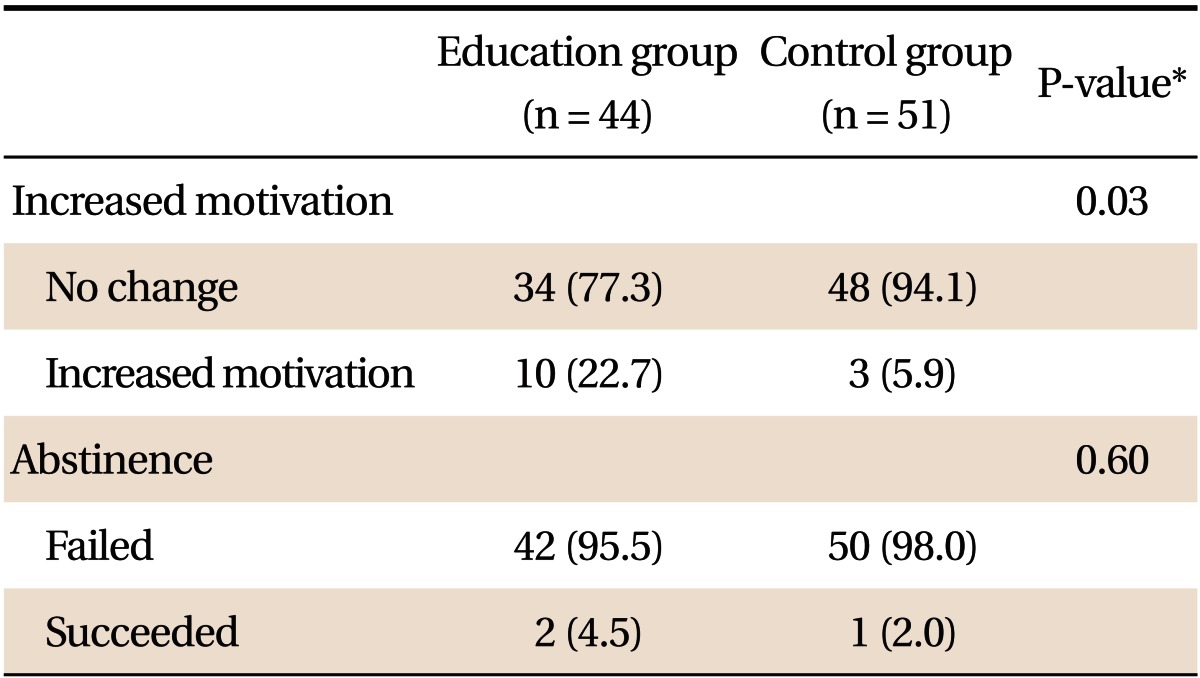
Table 2 illustrates the changes in the level of motivation to quit smoking and the rate of quitting smoking 4 weeks after smoking cessation education in both groups. A total of 10 subjects (76.9%) in the education group displayed improvement in the level of motivation to quit smoking, which was a significantly improved result in comparison to the 3 subjects (23.1%) in the control group (P = 0.03). However, only 2 subjects (66.7%) in the education group succeeded in quitting smoking 4 weeks later, which was more than the control group with 1 subject (33.3%) but did not have a significant change (P = 0.60).
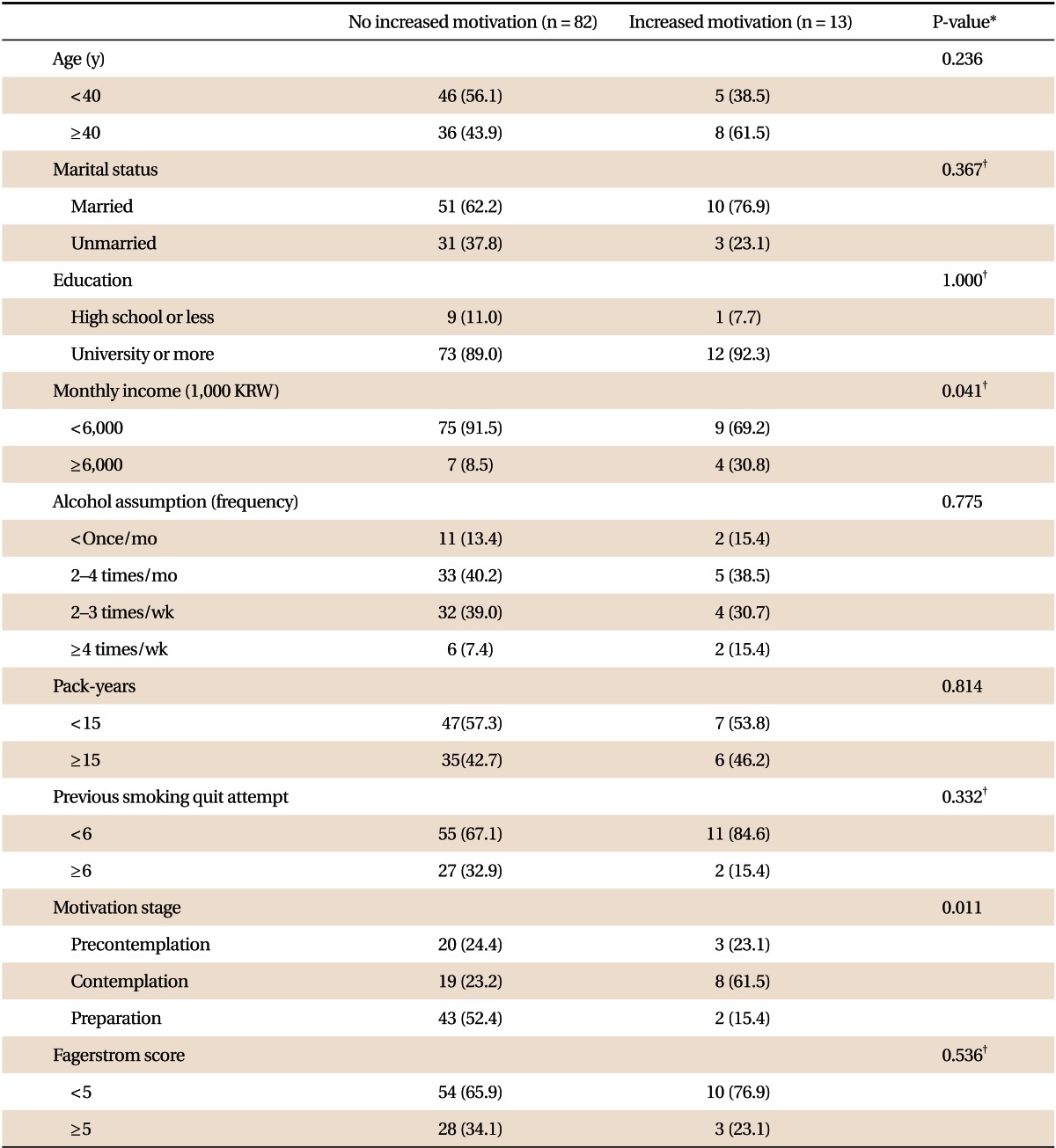
A variable with significant relevance to success in quitting smoking 4 weeks later was not found, while the variables that displayed significant relevance to the improvement in the level of motivation to quit smoking were found to be a monthly household income of more than 6 million Korean Won (P = 0.041) and an initial level of motivation to quit smoking (P = 0.011) (Table 3).
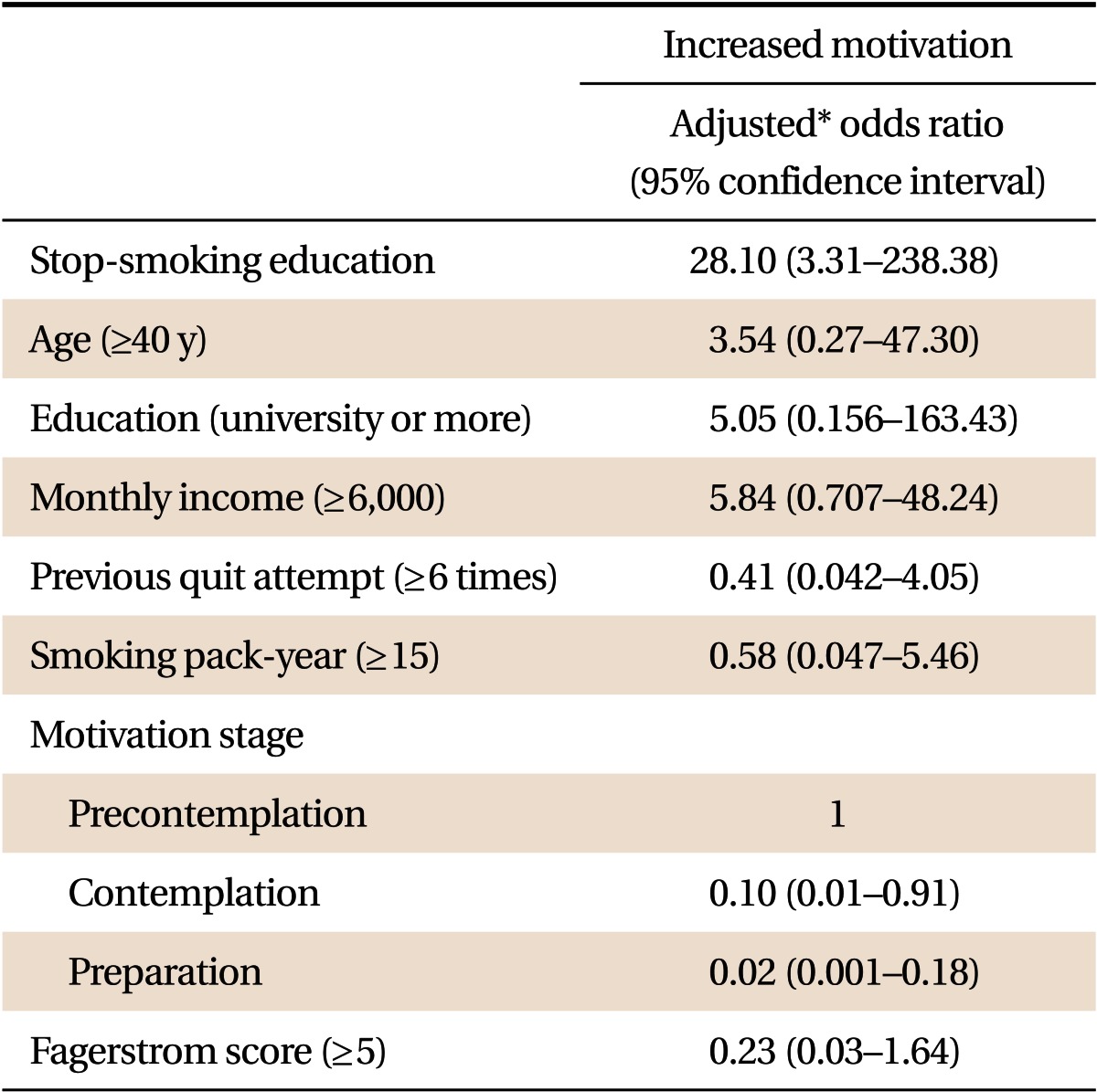
Multiple logistic regression analysis was carried out by including the variables that displayed significant differences between the education group and the control group (age, total number of cigarettes smoked, and Fagerstrom score). The variables that were found to be significant in the improvement of the level of motivation to quit smoking (monthly household income, initial level of motivation to quit smoking, educational level, and number of attempts made in the past to quit smoking for more than 24 hours) were also included in the multiple logistics regression analysis. The odds ratio that indicated success of quitting smoking for the education group was 4.34 times (95% confidence interval [CI], 0.29 to 65.87) higher than that of the control group but was not statistically significant (results are not shown). On the other hand, the odds ratio which indicated improvement in the level of motivation to quit smoking in the education group was found to be 28.10 times significantly higher than that of the control group (95% CI, 3.31 to 238.38) (Table 4).
DISCUSSION
This study was conducted outside, in public, with male smokers over the age of 19 who were office workers, and an improved motivation level to quit smoking after 4 weeks was observed even with simple smoking cessation education that took 5 to 10 minutes with measuring expiratory CO. However, there were no significant results regarding smoking cessation 4 weeks after the education session.
Numerous research has reported that smoking cessation education was effective in success13) and an improvement in the level of motivation to quit smoking.14,15) In this study, an improvement in the level of motivation to quit smoking was significantly higher in the education group as compared to the control group. However, success in quitting smoking was not significantly higher for the education group as compared to the control group because of the low intensity of education. According to research conducted on inpatients at Seoul Paik Hospital in Korea, a medical doctor carried out systematic smoking cessation education for 30 to 60 minutes with a focus on the diseases of the patients in the education group and gave short advice that lasted approximately 3 minutes for patients in the control group. When a telephone survey and additional education were carried out for 1 week, 1 month, and 3 months following discharge from the hospital, the rate of success for quitting smoking (37.1%) for the education group 3 months after discharge was significantly higher than the control group (14.3%).13) In the results of meta-analysis of 25 studies that conducted systematic smoking cessation education on inpatients and had a follow-up period of more than 6 months, the odds ratio for the improvement rate of quitting smoking following discharge in the education group was 1.37 times (95% CI, 1.27 to 1.48) higher than that of the control group.16) It was concluded that a short duration of smoking cessation education less than 10 minutes and a failure to conduct follow-up education are the major reasons for the lack of improvement in the success in quitting smoking in this study.
Secondly, the present study was carried out on adult male office workers who had not undergone a health check-up, hospitalization, or treatment at a smoking cessation clinic over the last 1 year. According to a domestic research study, the rate of quitting smoking 1 month after discharge without separate smoking cessation education during hospitalization was found to be 13.5%.7) In addition, the rate of quitting smoking for 143 smokers 6 months after the health check-up was 48%.6) The fact that subjects had not experienced affirmative situations for the motivation to quit smoking (such as hospitalization or health check-up) over the last 1 year was deemed to be the reason for the low success rate.
The small number of subjects in this study is another reason for the low success rate. According to research that examined the effect of a 5 to 10 minute smoking cessation program with 146 hospitalized orthopedic patients, the rate of success for smoking cessation for the education group 3 months after discharge was 16.9%, while that of control group was 6.7%.14) In this study, follow-up education was not carried out in the 4th week after discharge unlike the above research. However, the duration of initial education at 5 to 10 minutes was similar to the above the research and we believed that the visual information of the expiratory CO value, which was not provided in the aforementioned study, would elevate the educational effect. In addition, it was believed that the rate of smoking cessation could be elevated since the follow-up period (4 weeks) was short. So, the result of calculating the total number of subjects was 190 by setting the anticipated rate of quitting smoking at 25% with a level of significance at 0.05 and testability at 80% (composed of 95 from each of the groups). However, only 95 subjects were included in the study due to the limited research period and follow-up failure.
For the factors that affected the improvement in the level of motivation and success in quitting smoking, age did not display a significant relationship. While there were research results that reported that the rate of success in quitting smoking was higher with older age,17,18) there were also research results that reported the relevance lack of correlation between age and quitting smoking.19) Therefore, it was concluded that additional research is needed concerning the effect of age on the level of motivation and success in quitting smoking. In the majority of research, marital status has been known to be irrelevant to the success or the level of motivation to quit smoking.20) Marital status was also irrelevant in this study.
Although the rate of success in quitting smoking was known to be higher for higher educational levels,20,21) there was no significant relevance between the educational level and success or the level of motivation to quit smoking in this study. This result was thought to be due to the fact that the education level of the majority of the subjects in this study was higher than a bachelor' s degree. It was anticipated that results similar to existing research would be obtained if more subjects with an educational level lower than high school graduates were included.
When monthly household income was more than 6 million Korean Won, the level of motivation to quit smoking was found to be significantly higher than those with income level less than 6 million Korean Won. However, when other variables were adjusted, the odds ratio for increase in the level of motivation to quit smoking was 5.84 (95% CI, 0.707 to 48.24), failing to be a significant factor. Additional research is required due to the inconsistent results on the relationship between income and successful smoking cessation.13,22)
The results regarding the frequency of alcoholic consumption per week coincided with domestic research showing that there was no significant connection with success in quitting smoking.19) Although the connection between smoking and quantity of alcoholic consumption has been examined in numerous studies in Korea and overseas,17,21) this study failed to display a significant relationship. This may be because the frequency of alcoholic consumption per week failed to accurately reflect the total quantity of alcoholic consumption and alcohol consumption behavior, and given the characteristics of the subject population of male office workers, the frequency or quantity of alcoholic consumption was commonly high in both the group that displayed success or an improvement in the motivation to quit smoking and the group which did not. It is thought that there will be relevance between the quantity of alcoholic consumption and smoking if the daily quantity of alcoholic consumption were to be quantitatively assessed and analyzed.
Although existing research demonstrated that the total number of cigarettes of the smokers who succeeded in quitting smoking was lower than that of those who failed in quitting smoking, there was no significant difference between both groups in this study.21) It has been reported that the number of attempts to quit smoking in the past is not a significant variable, and this study also displayed the results that coincide with the existing reports.13,14,23)
It has been reported that the higher the initial level of motivation to quit smoking, the greater the improvement in the level of motivation and rate of success in quitting smoking following education.13,14) Although smoking cessation education using expiratory CO measurement did not have a significant relationship with the success in quitting smoking, a significant improvement in the level of motivation to quit smoking in this study could be deemed to support a substantial portion of previous research. However, when other variables were adjusted, the improvement in the level of motivation 4 weeks after the education dropped further with a higher level of motivation to quit smoking at the initial stage. This suggests that greater efforts are needed to improve the level of motivation with a higher initial level of motivation to quit smoking.
Nicotine dependence was higher in the group that failed to improve in the level of motivation to quit smoking, but it was not statistically significant. This result coincides with domestic research that there was no connection between success in quitting smoking and nicotine dependence,13,23) but there have also been numerous research studies that demonstrate that the higher the nicotine dependence, the greater the adverse effect on the success in quitting smoking due to the severity of withdrawal symptoms.14) Therefore, it was concluded that additional research is required on nicotine dependence, success in quitting smoking, and changes in the level of motivation.
The limitations to this study included the failure to conduct follow-up smoking cessation education and the difficulty in observing changes in the medium to long-term rate of success and the level of motivation to quit smoking, as the follow-up period was only 4 weeks. In addition, when determining the success in quitting smoking at the time of follow-up survey, this study failed to secure objective indices such as blood carboxyhemoglobin or expiratory CO values. Moreover it was not possible to observe the effectiveness of smoking cessation education in female and adolescent smokers as well as smokers working in other occupations. The small number of subjects was another limitation of this study.
However, in comparison to the fact that the existing research was conducted in an environment that has a positive influence on smoking cessation, such as inpatients and outpatients in a smoking cessation clinic, this study was carried out outside, in a public space, which was a neutral environment. Thus, we were able to assess the effectiveness of smoking cessation education itself more accurately. Moreover, it was the first research in Korea that demonstrated that improvement in the level of motivation to quit smoking could be induced by measuring expiratory CO values with simple smoking cessation education in an environment outside the hospital. Therefore, it is encouraging that this study has provided a clue for improving the level of motivation and success in quitting smoking in smokers for whom smoking cessation treatment has been ineffective due to their busy working schedule or other reasons.
If promotional activities for smoking cessation are conducted, such as developing other smoking cessation education methods and information materials that are convenient and placed effectively outside treatment rooms, the effectiveness and ability to improve the level of motivation and lower the rate of smoking can be anticipated. Smoking cessation would be much more successful if smokers with improved levels of motivation to quit smoking were brought into a smoking cessation clinics and drug therapy with repetitive outpatient consultation were carried out. We think that further research will be necessary for guiding smokers with improved motivation to smoking cessation treatment.