INTRODUCTION
Medical personnel may use a variety of questionnaires in order to discover alcohol use disorders at an early stage. There already exist a number of questionnaires for screening alcohol use disorders. The Michigan Alcoholism Screening Test questionnaire, CAGE (cutdown, annoyed, guilty, eye opener) questionnaire, and Alcohol Use Disorders Identification Test (AUDIT) questionnaire are the common examples.1-3) Among those questionnaires, the AUDIT questionnaire, which was developed by the World Health Organization (WHO), is composed of 10 questions; the first 3 questions address drinking frequency, amount of alcohol consumption and binge drinking, and the remaining 7 questions address alcohol problems. The questions addressing amount of alcohol consumption and frequency on the AUDIT are used to detect heavy drinking and binge drinking, and these are considered appropriate questions for evaluating alcohol problems among Koreans.4)
The AUDIT questionnaire was studied in Korea by Kim et al.4) in 1999, and it was mentioned that the questionnaire is more appropriate for discovering hazardous drinking habit at the early stages rather than diagnosing alcohol dependence. They suggested an AUDIT score of 12 points or more be referred to as problem drinking, 15 or more be referred to as an alcohol use disorder and 26 or more be referred to as alcohol dependence. In 2000, Lee et al.5) conducted a study on the Korean version of Alcohol Use Disorders Identification Test (AUDIT-K), and suggested that an AUDIT-K score of 12 or more should also be referred to as an alcohol use disorder.
Questions 1 and 2 of the AUDIT are used to measure the extent of heavy drinking and question 3 is used to measure the extent of binge drinking. The measures for calculating the number of standard drinks of alcohol used in questions 2 and 3 on the AUDIT are slightly unfamiliar to Korean people. The WHO3) dictates that 12 g of pure alcohol can be regarded as one standard drink. The National Institute on Alcohol Abuse and Alcoholism (NIAAA)6,7) of the United States defines 14 g of pure alcohol as one standard drink. Depending on the actual circumstances of each nation, if the amount consumed exceeds 60 g of pure alcohol, this can be referred to as binge drinking. Accordingly, the WHO3) dictates that over 5 standard drinks can be regarded as binge drinking and the NIAAA6) dictates that over 4 standard drinks can be regarded as binge drinking. The above Korean studies by Kim et al.4) and Lee et al.,5) however, did not mention the standard volume of the glass, but were conducted in accordance with the ABV of soju, the most public alcohol in Korea, at the time of the research. Soju prior to 1996 was an average of 25% to 35% ABV but soju which is manufactured currently is approximately 16.5% to 19.8% ABV.8) Therefore, the alcohol content itself has decreased, making the results of previous studies less applicable. Moreover, the AUDIT questionnaires of the previous generation in Korea did not introduce the concept of the standard drink in questions 2 and 3, and this may lead to an inappropriate measurement in comparison to today's soju with regard to heavy drinking and binge drinking.
When questioned about the number of glasses consumed, Koreans tend to assume that the question is based on the soju glass or the beer glass. A quarter bottle of soju or 500 mL of beer consist of 14 g of pure alcohol. Therefore, there needs to be an amendment to question 2 and 3 of the AUDIT questionnaire in order to make it more precise. In company with the introduction of the concept of standard drinks in question 2 and 3, the cutoff value for screening alcohol use disorders and at-risk drinking in the AUDIT questionnaire is expected to be changed. Kim et al.9) suggested the use of a new AUDIT-Korean revised version (AUDIT-KR) that would reflect the recent changes of alcohol concentration in Korean liquor. The AUDIT-KR explains the standard drink for each type of liquor in simple and easy terms so that Koreans can understand it easily. There has not been, however, any research on the reliability and validity of the AUDIT-KR yet. Therefore, this study was performed to examine the reliability, validity, and appropriate cutoff values of the AUDIT-KR.
METHODS
1. Subjects
The present study was conducted on 435 respondents who agreed to take part in the questionnaire (210 males and 225 females), excluding 65 out of 500 respondents (250 males and 250 females) who did not fully complete the AUDIT-KR questionnaire. The respondents were patients under the age of 65 who visited the Health Promotion Center of Chungnam National University Hospital for a comprehensive medical examination from January 2012 to June 2012.
2. Collection of Data
Gender, age, and smoking status were examined by the self-administered questionnaires. Ten questions of the AUDIT-KR were answered by the respondents. Scoring on the AUDIT-KR followed the same procedure as the AUDIT questionnaire, which allocated 4 points for each question, thus having a total of 40 points. Apart from the questionnaires, there was a personal interview in order to diagnose at-risk drinking and alcohol use disorders. In the current study, at-risk drinking was defined as heavy drinking or binge drinking according to the guidelines issued by the NIAAA.6,7) More than 14 standard drinks (one standard drink = 14 g of alcohol) a week for males and more than 7 standard drinks a week for females were considered heavy drinking. More than 4 standard drinks for males and more than 3 standard drinks for females at a drinking session were considered binge drinking. Alcohol use disorders (alcohol abuse and alcohol dependence) were diagnosed by the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, tex revision10) from the structured interview of medical examiners.
3. Changes in the AUDIT-KR Questionnaire
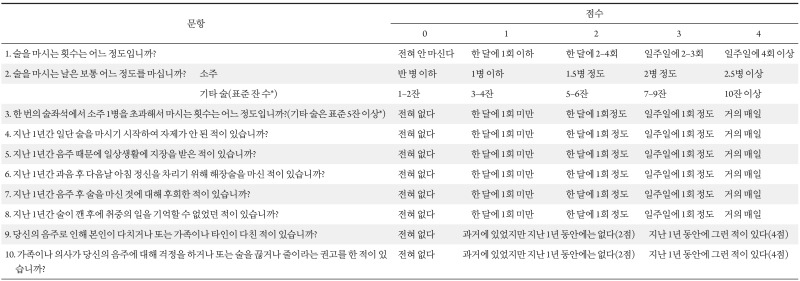
The AUDIT-KR (Appendix 1) used in the present study was slight different from the questionnaires of the AUDIT which were translated by Kim11) in 1998 or the questionnaires of the AUDIT-K which was studied by Lee et al.5) in 2000. The differences can be found in questions 2, 3, and 10. Question 2 in Kim's translated version and Lee et al.'s AUDIT-K used the number of glasses for each liquor type, while the AUDIT-KR of the current study used the concept of the standard drink of 14 g of alcohol by reflecting the decrease in the concentration of soju. In question 3 for binge drinking status, Kim's translation and Lee et al.'s AUDIT-K stated 'equal to or more than' one bottle of soju (or 4 bottles of beer) at a single drinking session, while the AUDIT-KR stated 'more than' one bottle of soju or '5 or more' standard drinks (other liquor). The changes in question 3 of the AUDIT-KR reflect the guidelines suggested by the NIAAA6) which defines consumption of more than 60 g of alcohol as binge drinking. In question 10 where it asks if relatives, friends or doctors have advised the subject to stop drinking, the multiple choices of Kim's translation and the AUDIT-KR of this study are identical to the ones that the WHO uses: 1) 'never (0 point),' 2) 'I have not been advised during the last one year but I was before then (2 points),' 3) 'Yes, I have been advised during the last one year (4 points).' On the other hand, the AUDIT-K of Lee et al. uses: 1) 'never (0 point),' 2) 'less than once a month (1 point),' 3) 'once a month (2 points),' 4) 'once a week (3 points),' 5) 'everyday (4 points),' which may result in lower points than the original AUDIT.
4. Data Analysis
Sociodemographic features of respondents were presented as averages and percentage ratio, and gender difference were studied as well. Among the general characteristics of the subjects, the AUDIT-KR score was compared between genders by the Wilcoxon-rank sum test because it did not show normal distribution, and the median values and the interquartile range were presented. Other characteristics were compared by t-test and chi-square test. The respondents with at-risk drinking, alcohol abuse, and alcohol dependence were identified. In order to evaluate the reliability of the AUDIT-KR, Cronbach's alpha coefficient was computed. The area under the receiver operating characteristic curve (AUROC) of the AUDIT-KR was obtained in order to identify at-risk drinking and alcohol use disorders. The sensitivity and specificity of each cutoff value were calculated. The cutoff value having the biggest Youden index, which is the sum of sensitivity and specificity, was suggested as an appropriate cutoff value. IBM SPSS ver. 20.0 (IBM Co., Armonk, NY, USA) was used as the statistical program and the definition of significance was limited to P-values lower than 0.05.
RESULTS
1. General Characteristics of Subjects
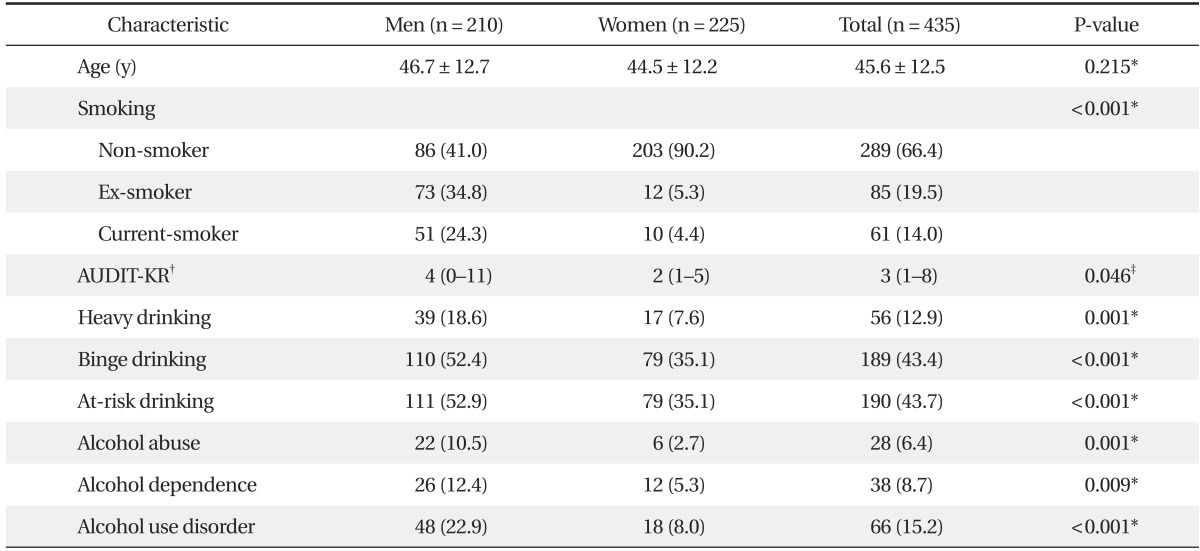
The mean ± SD age of the total subjects was 45.6 ± 12.5, 46.7 ± 12.7 years for males and 44.5 ± 12.2 for females and there was no significant difference between genders (P = 0.215). Smoking status of males was significantly higher (P < 0.001) than females. The mean ± SD AUDIT-KR score of the total subjects was 5.59 ± 6.53, having a median value of 3 and an interquartile range of 1 to 8. The mean ± SD AUDIT-KR score of males was 6.87 ± 7.68, having a median of 4 and an interquartile range of 0 to 11. The mean ± SD AUDIT-KR score of females was 4.26 ± 4.74, having a median of 2 and an interquartile range of 1 to 5. Males showed significantly (P = 0.046) higher AUDIT-KR score than females. Fifty six respondents (12.9%) were identified as heavy drinking (39 male and 17 female), 189 respondents (43.4%) were identified as binge drinking (110 male and 79 female), 190 respondents (43.7%) were diagnosed with at-risk drinking (111 male and 79 female), 28 (6.4%) were diagnosed with alcohol abuse (22 male and 6 female), 38 (8.7%) were diagnosed with alcohol dependence (26 male and 12 female), and 66 (15.2%) were diagnosed with alcohol use disorders (48 male and 8 female) (Table 1).
2. Validity and Cutoff Value of the AUDIT-KR in Screening At-risk Drinking
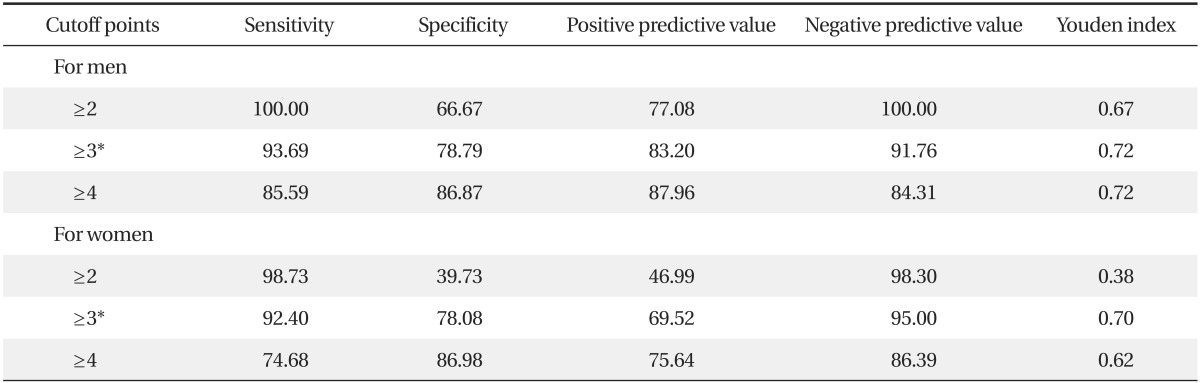
Cronbach's alpha of the AUDIT-KR was 0.885 which suggested high reliability. AUROC (95% confidence interval [CI]) of the AUDIT-KR in screening at-risk drinking was 0.946 (0.918-0.975) for males and 0.898 (0.857-0.939) for females. An appropriate cutoff value for screening at-risk drinking was 3 points in both males and females. At the value of 3 points, sensitivity and specificity of the AUDIT-KR was 93.69% and 78.79%, respectively, in males, and 92.40% and 78.08%, respectively, in females (Table 2, Figure 1).
3. Validity and Cutoff Value of the AUDIT-KR in Screening Alcohol Use Disorders
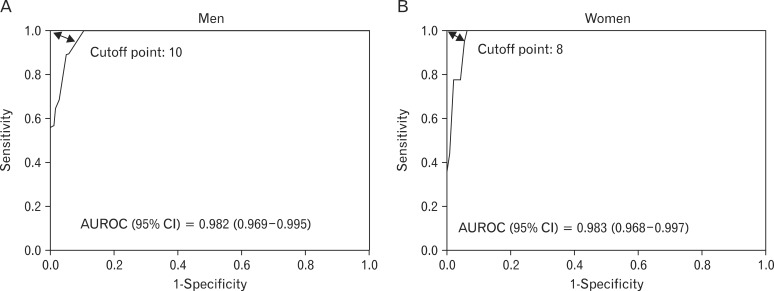
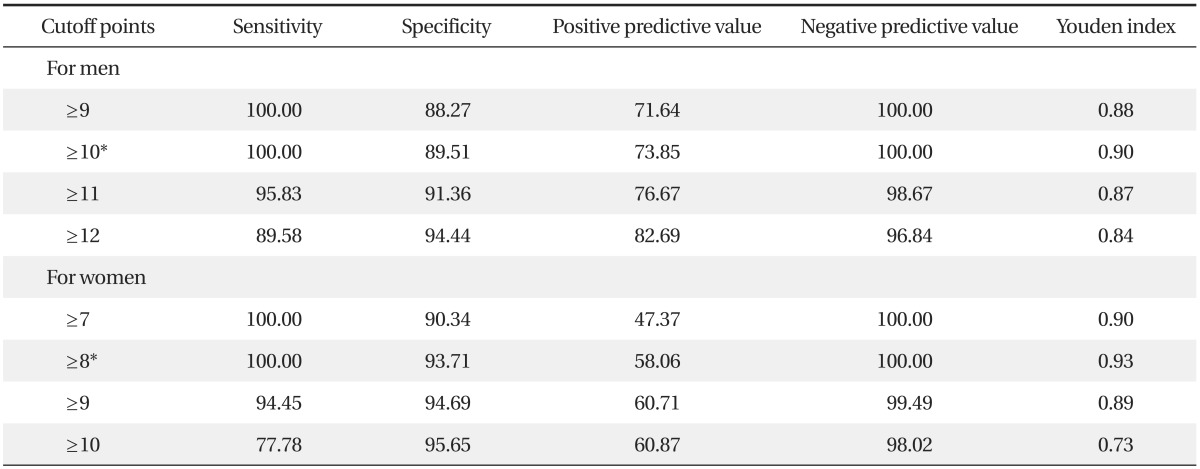
The AUROC (95% CI) of the AUDIT-KR in screening alcohol use disorders was 0.982 (0.969-0.995) for males and 0.983 (0.968-0.997) for females. An appropriate cutoff value for screening alcohol use disorders was 10 points for males and 8 points for females. At the value of 10 points, sensitivity and specificity of the AUDIT-KR was 100.00% and 89.51%, respectively, in males. At the value of 8 points, sensitivity and specificity of the AUDIT-KR was 100.00% and 93.71%, respectively, in females (Table 3, Figure 2).
DISCUSSION
While it is important to provide a cure to patients with alcohol use disorders in primary care, it may be more constructive to screen as a preventive measure against future alcohol abuse. In order to establish effective intervention strategies at the early stages of alcohol problems in primary care practice, there should be an effective screening tool which is able to identify patients who have drinking problems. The present study may be considered meaningful in that the AUDIT-KR was confirmed for its sufficient sensitivity and specificity with reliability. In addition, the current study suggests the cutoff value for screening at-risk drinking and alcohol use disorders in accordance with changes in the ABV of liquor in Korea.
When screening at-risk drinking, the results of this study suggest 3 points as an appropriate cutoff value of the AUDIT-KR for males and females. The appropriate cutoff value of the AUDIT-KR for screening alcohol use disorder was suggested as 10 points in males and 8 points in females. The cutoff value suggested in the present study was slightly lower than the ones that Kim et al.4) suggested, 12 points for problem drinking, 15 for alcohol use disorders, and 26 for alcohol dependence.
The reason behind this discrepancy may have resulted from the difference in the scores of questions 2 and 3 in the AUDIT questionnaire. The AUDIT-KR of the current study reflects the concept of standard drinks that is not a part of the AUDIT questionnaire which had been used in Kim et al.'s study. In other words, if one drinks 7 glasses of soju, he or she would get 3 points for question 2 in the previous Korean AUDIT questionnaire, while he or she would only get 1 point for the same question in the AUDIT-KR questionnaire, because it now reflects the concept of the standard drink which calculates 7 glasses of soju as equivalent to 4 standard drinks. In addition, reflecting the changes in question 3 of the previous AUDIT from 'equal to or more than' 1 bottle of soju to 'more than' 1 bottle of soju in the AUDIT-KR may also have produced the difference. Moreover, in the previous Korean version of the AUDIT questionnaire, questions 3 to 8 had created some confusion in their multiple choices where option 1 was 'less than or equal to once a month' and option 2 was 'approximately once a month.' The AUDIT-KR, however, changed these options to make it more clear, with option 1 now reading 'less than once a month' and option 2 reading 'once a month,' which may have lowered the cutoff value.
Meanwhile, the WHO3) suggests that a cutoff value greater than 8 points may indicate alcohol problems including alcohol dependence. In a number of studies conducted all around the world which studied the cutoff value of the AUDIT, a low cutoff value for alcohol use disorder and alcohol dependence was suggested.12-16) Tsai et al.12) conducted research on the AUDIT among Chinese inpatients and suggested a cutoff value of 8 points for harmful use and 11 for alcohol dependence in 2005. Dybek et al.13) conducted a study on the AUDIT among German people and suggested a cutoff value of 8 points for alcohol use disorder in 2006. Moussas et al.14) suggested a cutoff value of 8 points for alcohol dependence among Greek patients in 2009. Pradhan et al.15) suggested a cutoff value of 9 points for alcohol use disorder and 11 for alcohol dependence on its Nepalese in 2012. Our results also suggest a low cutoff value just like the studies mentioned above.
The cutoff value of the AUDIT for at-risk drinking was suggested as 8 points for males ≤ age 60, and 4 points for females and males > age 60.16-18) There were, however, not enough references for the cutoff values for at-risk drinking in Korea. The results of the study by Lee et al.19) on the problem drinking of college students suggested that the cutoff value should be 8 points for males and 6 for females, and a Nigerian study suggested a cutoff value for at-risk drinking of college students of 5 points.20) A study on senior citizens by Ryou et al.21) suggested 7 points as a cutoff value for screening for geriatric problem drinking. In the present study, 3 points was suggested for both males and females, which is a lower cutoff value than the one suggested by previous studies. The fact that respondents in the current study reported more of binge drinking than heavy drinking may be a factor behind this discrepancy. The frequency of binge drinking may be higher in Korea than that of any other country and the cutoff value could be specified lower.22) While questions 1 and 2 on the AUDIT questionnaire are related to heavy drinking, question 3 is related to binge drinking. Therefore, it is possible for one to have a lower score if he or she answered positively on question 3 because he or she may be negative on questions 1 and 2. Therefore, the results of this study may be different from the previous ones. In comparison to the previous studies, however, the cutoff values have been lowered and the advantage lies here where at-risk drinking and alcohol use disorders can be detected at the early stages.
There are some limitations in generalizing the results of our study. First, the subjects of the present study were limited to patients from only one hospital. Additionally, the respondents of the current study came to the hospital for a physical check-up and there may have been a number of family members with them, which would have encouraged them to answer the questions with a lower volume of alcohol than their actual intake. Therefore, future studies targeting a larger sample size and respondents with various characteristics should be conducted. According to a Korean epidemiological investigation on mental diseases in 2011, the prevalence rate of alcohol use disorders was 20.7% for males and 6.1% for females, and the total was 13.4%.23) The prevalence rate of alcohol use disorders in this study was slightly higher (22.9% for males, 8.0% for females, and 15.2% for a total) than the average statistics of Korea. The fact that those with drinking problems were more involved in our study is another limitation to generalizing the results. Finally, the present study did not show any other sociodemographic features than age, gender, or smoking status.
In spite of these limitations, it is meaningful that the current study suggests a new cutoff value upon having proven the validity and reliability of the AUDIT-KR which reflects the true Korean situation more accurately. In addition, our study suggested the cutoff values for each gender, which were not conducted in the previous studies. Moreover, by using the amended questions in the AUDIT-KR, the concept of standard drinks suggested by the WHO and NIAAA will be precisely reflected. More appropriate drinking evaluation will be available in primary care in accordance with the international criteria of heavy drinking and binge drinking. Through additional studies using the AUDIT-KR, cutoff values will be verified in order to screen at-risk drinking and alcohol use disorders.