INTRODUCTION
Sedentary lifestyles have become common over the past few decades with the modernization of the society.1) Sedentary behavior, which is distinct from physical inactivity, is defined as a failure to meet the current physical activity recommendations.2) Individuals who meet the current physical activity recommendations may also have negative health outcomes if they spend excessive time sitting. The Korea Ministry of Health and Welfare recommends less than 2 h/d of sitting time and performing slight physical activities. At least 10 minutes per one bout of moderate-to-vigorous physical activity (MVPA) is also recommended. 3)
Numerous studies suggest that high amounts of sedentary behavior are associated with increased risk of morbidity and mortality regardless of MVPA level.2) Increasing evidences show that sedentary behavior is an independent risk factor of cardiovascular disease regardless of MVPA.4) A previous study found linear associations between sedentary time and low high-density lipoprotein (HDL) cholesterol, as well as high triglycerides, waist circumference, C-reactive protein, and insulin. 5) Similarly, consistent positive associations between all sedentary behaviors and triglycerides, low-density lipoprotein (LDL) cholesterol, or total cholesterol were observed in normal weight individuals.6) In contrast, a recent study has suggested that cardiovascular disease risk is non-linearly associated with sedentary time with an increased risk only at extremely high levels (>10 h/d).7) Another study found no associations between cardiovascular biomarkers and sedentary time.8) A study among Korean children and adolescents, aged 12 to 18 years, found that watching TV is significantly associated with risks of overweight, high abdominal adiposity, and low HDL cholesterol; an additional hour spent playing video games also increases the risk of high abdominal adiposity.9)
Few studies about the associations between sedentary time and cardiovascular risks among Korean adults have been conducted. Therefore, we examined the associations between sedentary time and cardiovascular risk factors in a large representative sample of Korean adults in this study.
METHODS
1. Participants
Data were collected from the 2013 Korean National Health and Nutrition Examination Survey (KNHANES) VI. The KNHANES is a nationwide cross-sectional survey designed to gather information on the sociodemographic status, health examination, and health behaviors, including physical activities, among representative samples of Koreans. To sample representative individuals of the civilian, non-institutionalized Korean population, we used a complex multistage probability sampling design. Among the 8,018 individuals participated in 2013 KNHANES, we included 6,273 participants aged 19 years and above. Patients who had no information on sedentary time (n=934) and pregnant women (n=31) were excluded from the analyses. Those who were diagnosed with hypertension, diabetes, dyslipidemia, stroke, myocardial infarction, angina, osteoarthritis, rheumatoid arthritis, and any cancers (n=2,007) were also excluded to reduce the possibility of reverse-causality. Data from 3,301 participants were available for the present analysis.
2. Measurements
1) Cardiovascular risk factors
Biomarkers of cardiovascular risk included systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol, HDL cholesterol, LDL cholesterol, triglycerides, and fasting glucose. Blood pressure was measured 3 times after at least 5 minutes of rest in a sitting position with a mercury sphygmomanometer by a trained staff. Mean SBP and DBP were calculated as the mean of the last 2 measurements. Total cholesterol and triglycerides were measured with the enzymatic method. HDL cholesterol and LDL cholesterol levels were measured using the homogeneous enzymatic colorimetric method. Fasting glucose level was measured with the hexokinase method. All laboratory tests were performed with COBAS 8000 C702 (Roche, Mannheim, Germany). Measurements with 8 or more fasting hours (12 hours for triglycerides) were used for analyses. Direct LDL cholesterol level was measured when triglyceride levels were higher than 200 mg/dL, and calculated LDL cholesterol level was obtained using the Friedewald equation only when triglyceride levels were <200 mg/dL. In this study, we performed either direct or calculated measurements. Measurements of cardiovascular biomarkers were categorized into dichotomous variables according to the Adult Treatment Panel (ATP) III criteria. High SBP was defined as 130 mm Hg or higher, and high DBP was defined as 85 mm Hg or higher. High SBP or DBP is considered high blood pressure. High total cholesterol level was defined as 200 mg/dL or higher. A cholesterol level of less than 40 mg/dL in men or less than 50 mg/dL in women indicates a low HDL cholesterol. High triglyceride and high LDL cholesterol levels were defined as 150 mg/dL or higher and as 130 mg/dL or higher, respectively. A glucose level of 100 mg/dL or higher is considered high fasting glucose level.
2) Sedentary time and physical activity
Sedentary time and physical activities (vigorous, moderate, and walking) were assessed by self-reported questionnaire based on the International Physical Activity Questionnaire (IPAQ). Participants were asked the question: ŌĆ£How much time do you usually spend sitting on a typical day for the last seven days (min/d)?ŌĆØ Total sedentary time per day was used as both continuous and categorical (quintile) variables. Quintile cutoff points for the total sedentary time were 3.0, 4.5, 6.0, and 9.5 h/d. MVPA (metabolic equivalent of task [MET]-min/wk) was calculated using the guideline for data processing and analysis of the IPAQ short form10) and was then categorized into tertiles.
3) Other covariates
The following sociodemographic and lifestyle covariates were considered as possible confounders: age, sex, education level (below high school/high school/above high school), income level (quartiles), marital status (married/single/others), type of occupation (inactive/active), residence (urban/rural), menopausal status (premenopause/menopause), smoking status (non-smoker/ex-smoker/current smoker), alcohol use (none/moderate/heavy), calorie intake (tertiles), body mass index (BMI, low to normal/overweight/obese), and waist circumference (normal/abdominal obesity).
Income levels were categorized into quartiles using monthly average household equivalent income (monthly average household income/square root of number of household members) by sex and age groups. Marital status was categorized into married, single, and others (bereaved, divorced, separated, or no response). Types of occupation were dichotomized into inactive and active jobs from seven job categories based on MVPA of each category. Inactive jobs included manager, specialist, office worker, and unemployed (housewife, student); active jobs included service worker and seller, foster and fishery worker, machine operator, assembler, and simple labor worker. Participants who had smoked less than 100 cigarettes in their entire lives were regarded as non-smoker. Alcohol use groups were classified according to the National Institute on Alcohol Abuse and Alcoholism criteria.11) Calorie intake was categorized into tertiles, and no data group on nutrition existed. BMI was calculated by weight divided by the square of height. The cutoff points for overweight and obesity were 23 and 25 kg/m2, respectively, based on the criteria for Asians. Waist circumference cutoff points were 90 cm in men and 85 cm in women.
4) Statistical analysis
Weights and sample design variables were applied in analyses to take into account a complex, multistage, probability sampling design of KNHANES. Weighted descriptive characteristics (means, standard errors, proportions) were calculated using the guideline for 2013 KNHANES analysis. To compare sociodemographic variables by sex, we conducted t-tests and chi-square tests. Dependent variables (SBP, DBP, total cholesterol, HDL cholesterol, triglycerides, LDL cholesterol, and fasting glucose) were categorized into dichotomous variables according to the ATP III criteria. Self-reported sedentary time was analyzed as continuous and categorical variables (quintiles). Multivariate logistic regression was performed with adjustment for age, sex, education level, income level, marital status, type of occupation, residence, menopausal status, smoking status, alcohol use, calorie intake, BMI, waist circumference, and MVPA. All statistical analyses were performed using Stata ver. 14.1 for Windows (Stata Corp., College Station, TX, USA). P<0.05 was considered statistically significant.
RESULTS
1. Characteristics of Study Participants
The mean┬▒standard error age of the 3,301 participants was 39.5┬▒0.3 years. The mean sedentary time among participants was 6.1 h/d (6.3 h/d in men, 6.0 h/d in women; P<0.05) (Table 1). Men reported more practice of MVPA than women (P<0.001). The average BMI was 24.1 kg/m2 in men and 22.5 kg/m2 in women (P<0.001). The proportion of abdominal obesity was higher in men (20.0%) than in women (11.6%) (P<0.001).
2. Cardiovascular Risk Factors
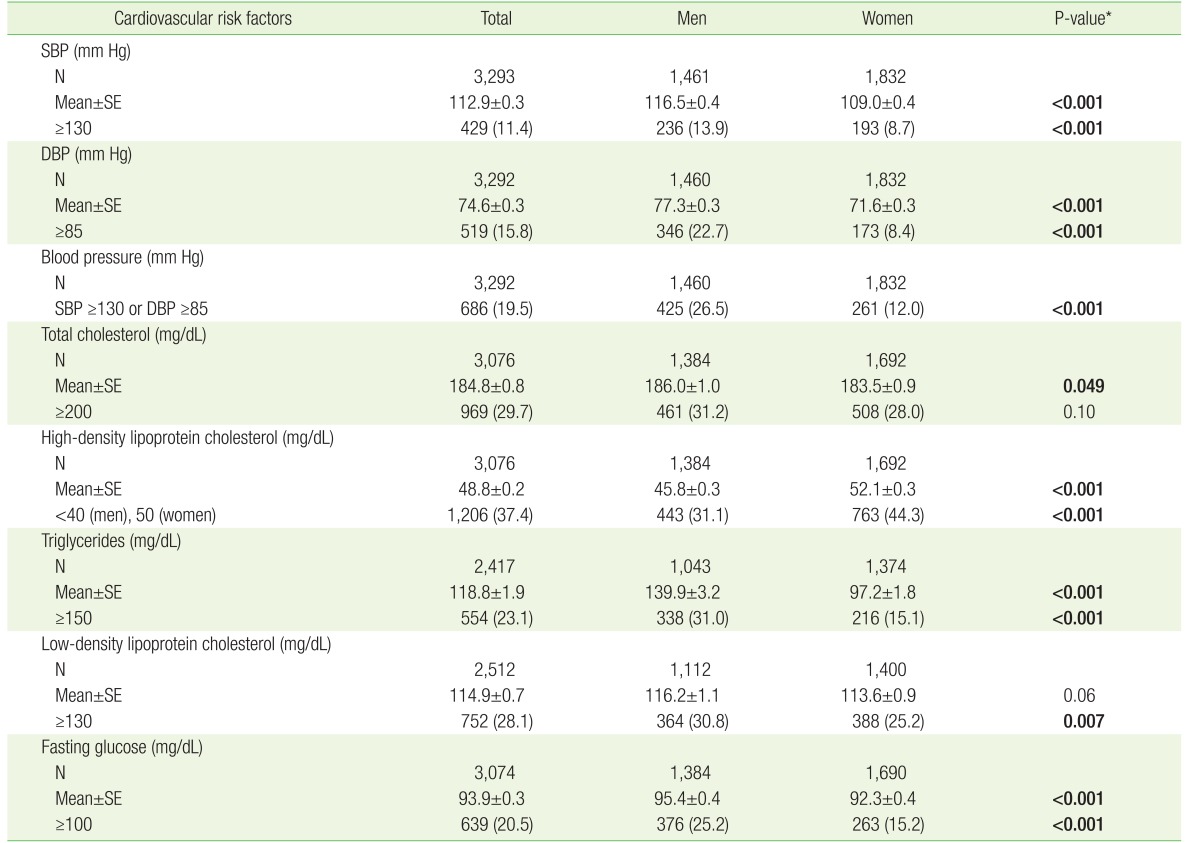
The mean values of SBP and DBP were higher in men than in women (P<0.001) (Table 2). Similarly, the proportions of high SBP, high DBP, or high blood pressure were higher in men than in women (P<0.001). Compared with women, men exhibited higher mean values and proportions of abnormal levels for most of the lipid profiles and fasting glucose. However, the proportion of low HDL cholesterol was higher in women than in men (P<0.001).
3. Sedentary Time and Cardiovascular Risk Factors
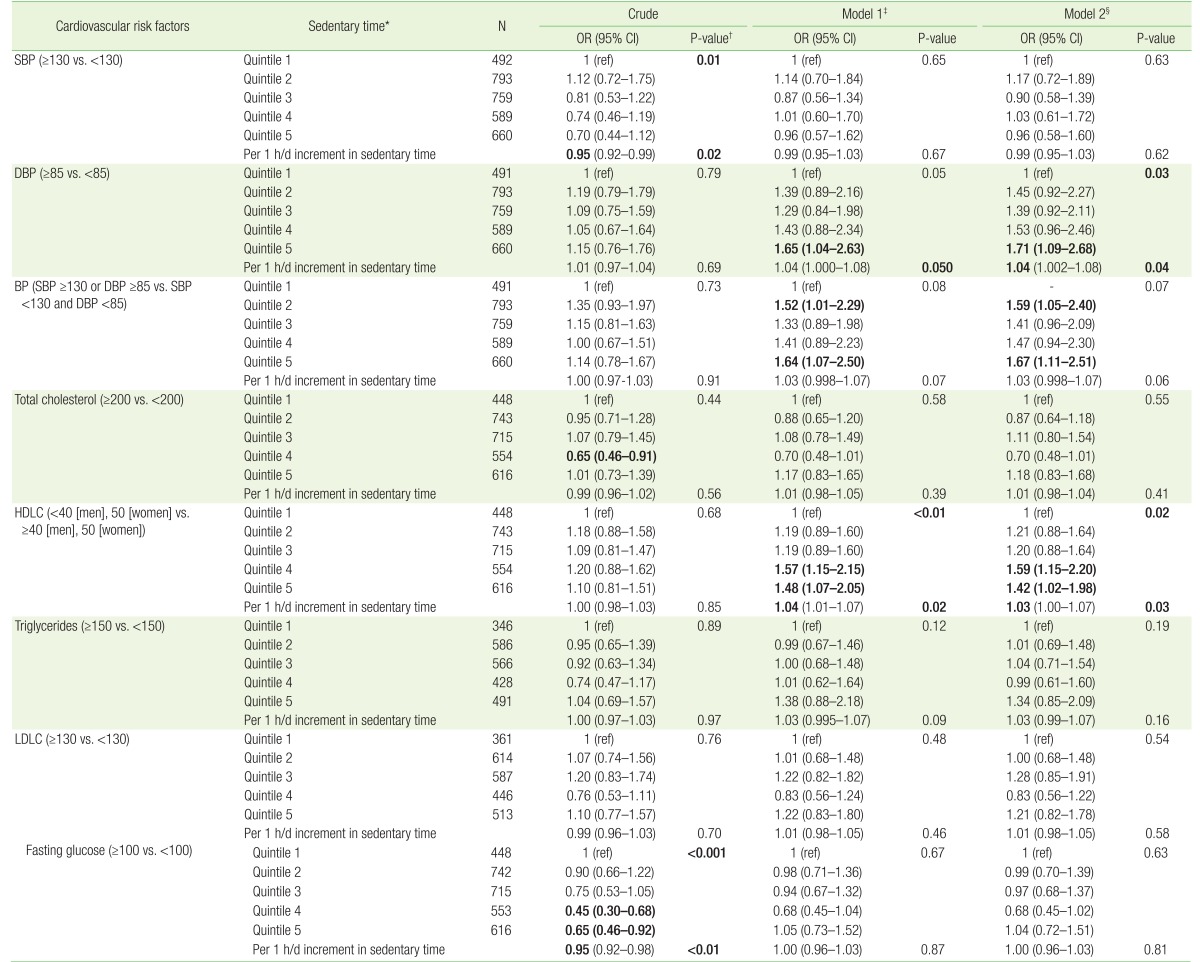
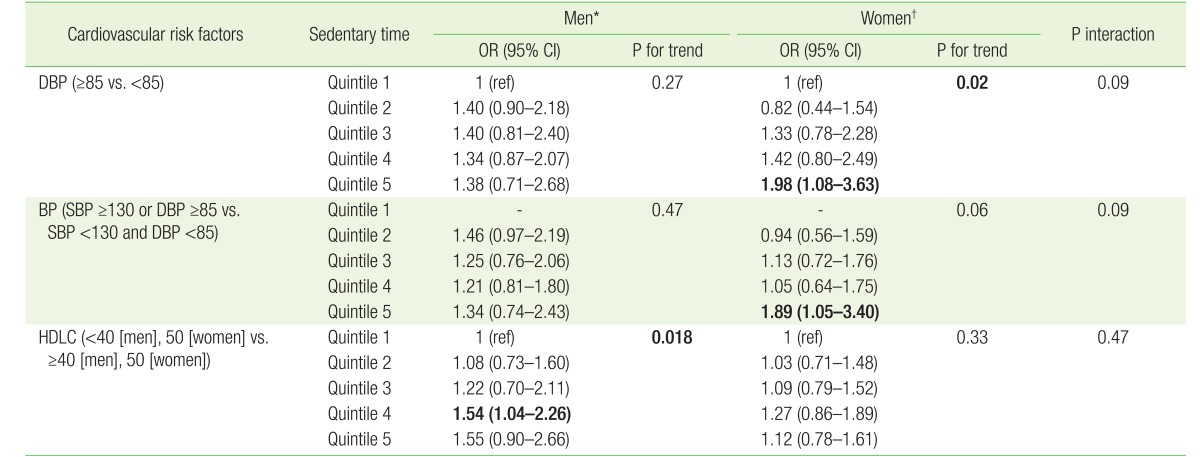
Sedentary time was inversely associated with SBP (top versus bottom quintile: adjusted odds ratio [aOR], 0.70; 95% confidence interval [CI], 0.44 to 1.12; Ptrend=0.01) and fasting glucose (top versus bottom quintile: aOR, 0.65; 95% CI, 0.46 to 0.92; Ptrend <0.001) before adjustment (Table 3). However, after adjustment for age, sex, education level, income level, marital status, type of occupation, residence, menopausal status, smoking status, alcohol use, and calorie intake (model 1), the associations with both SBP and fasting glucose were attenuated (Ptrend=0.65, Ptrend=0.67). In model 1, high DBP and low HDL cholesterol were significantly associated with prolonged sedentary time (for high DBP, top versus bottom quintile: aOR, 1.65; 95% CI, 1.04 to 2.63; Ptrend=0.05; for low HDL cholesterol, top versus bottom quintile: aOR, 1.48; 95% CI, 1.07 to 2.05; Ptrend<0.01). These associations remained significant even after further adjustment for BMI, waist circumference, and MVPA (model 2). For high DBP, the top versus bottom quintile aOR was 1.71 (95% CI, 1.09 to 2.68; Ptrend=0.03). For low HDL cholesterol, the top versus bottom quintile aOR was 1.42 (95% CI, 1.02 to 1.98; Ptrend=0.02). When sedentary time was used as a continuous variable, per 1-hour increment in sedentary time per day was significantly associated with elevated DBP and low HDL cholesterol level. The aOR of elevated DBP was 1.04 (95% CI, 1.00 to 1.08; P=0.04), and the aOR of low HDL cholesterol was 1.03 (95% CI, 1.00 to 1.07; P=0.03). We found no significant associations between sedentary time and other cardiovascular risk factors. When the associations were further stratified by sex, the associations between sedentary time and cardiovascular risk factors were similar in both sexes (Pinteraction Ōēź0.05) (Table 4).
We performed several sensitivity analyses and found almost similar results to the main analyses. When confounding variables (BMI, waist circumference, physical activity) were used as continuous variables, the associations of sedentary time with DBP (Ptrend=0.03) and HDL cholesterol (Ptrend=0.01) were similar to the main results. In addition, when MVPA levels were categorized using the World Health Organization criteria (<600, 600ŌĆō3,000, Ōēź3,000 METs), the associations of sedentary time with DBP (Ptrend=0.03) and HDL cholesterol (Ptrend=0.01) were similar to the main results.
DISCUSSION
In this cross-sectional study, prolonged sedentary time was significantly associated with high DBP and low HDL cholesterol in Korean adults. These associations were independent of general and abdominal obesity and MVPA levels.
Similar to a previous study,12) we found that sedentary time was significantly associated with DBP, but not with SBP. The biological mechanisms that may explain the observed association between sedentary behavior and DBP remain unclear. One possibility is that sedentary behavior may affect blood pressure in different ways, and SBP can be affected by changes in peripheral vascular resistance to a much lesser extent than DBP.12)
Numerous studies5)6)8)13) and the present study found that prolonged sedentary time is associated with low HDL cholesterol. A study among adults aged 30ŌĆō50 years reported that sedentary time is associated with HDL cholesterol, but not with other lipid profiles or blood pressure. 8) Although we found no significant association with triglycerides, some studies, including a meta-analysis, reported significant associations with triglycerides.5)6)13)14) In the meta-analysis of studies using accelerometer, only triglycerides were associated with sedentary time among the lipid profiles.14) As a plausible mechanism, prolonged sedentary behavior suppresses the activities of lipoprotein lipase-a protein important for controlling plasma triglyceride catabolism, HDL cholesterol, and other metabolic risk factors. Low lipoprotein lipase is associated with blunted plasma triglyceride uptake and reduced plasma HDL cholesterol levels.15)
In contrast to our study, several studies reported significant associations between sedentary time and glucose- and insulin-related markers.5)8)16)17) A study among Latino/Hispanic adults found that sedentary time is associated with fasting and 2-hour glucose, as well as fasting insulin and homeostatic model assessment of insulin resistance, after exclusion of individuals who were diagnosed with or taking medications for cardiovascular disease.13) An animal study reported a decline in whole-body insulin sensitivity and an increase in visceral fat amount when physically active rats stop high levels of exercise.18)
No gold standard for sedentary behavior assessment has been established.19) In this study, we measured sedentary time using a standardized self-administered questionnaire. Recent studies suggested that quantification of sedentary time and physical activity is necessary, such as by using an accelerometer. Another point is that patterns of sedentary time may have differential effects on cardiovascular risks. A study in a large representative sample of Canadian adults reported that breaking-up sedentary time is more related to cardio-metabolic variables than total sedentary time.16) A recent study found that the association between sedentary time and cardio-metabolic risks becomes insignificant after adjustment for overall physical activity measured using an accelerometer, instead of MVPA.20) Sedentary behavior usually refers to any waking behavior characterized by an energy expenditure Ōēż1.5 MET.2) No currently used questionnaires assess physical activity levels between 1.5 METs (sedentary activity) and 3.0 METs (moderate physical activity). Thus, this study suggests that sedentary behavior may not have health effects independent of physical activity if overall physical activity is adjusted. In addition, types of sedentary activities may have different health effects. A recent large prospective study found that watching TV is associated with an increased cardiovascular mortality; however, time spent sitting in a car or bus and at work is not related to mortality. This finding proposes that sedentary behavior may consist of different natures.21)
The present study has several strengths. To the best of our knowledge, this study is the first to investigate relationships between sedentary time and cardiovascular risk factors in a large representative sample of Korean adults. We applied sample design variables and weights in analyses to represent the entire Korean population. We also adjusted for various sociodemographic and health-related variables that may affect the relationships between sedentary time and cardio-metabolic risk factors.22) Compared with most of the previous studies that included individuals with preexisting cardiovascular disease and adjusted for the disease histories, we excluded those who were diagnosed with cardio-metabolic diseases or cancers to reduce reverse-causality between sedentary time and cardio-metabolic markers.
The potential limitations of this study are as follows. First, we used self-reported data on sedentary time and physical activity assessed using IPAQ, a validated and widespread questionnaire.23) However, we cannot exclude the possibility that using self-report to quantify activity may underestimate the strength of relationships with risk factors.24) Another issue is that no currently used questionnaires measure 1.5ŌĆō3.0 METs of physical activities. Second, we did not evaluate the effects of breaking-up sedentary time. Lastly, this was a cross-sectional study; the design precluded casual inferences about the relationships.
In conclusion, prolonged sedentary time was significantly associated with high DBP and low HDL cholesterol level in Korean adults. The associations were independent of general and abdominal obesity and MVPA levels. Future longitudinal investigations on the association between sedentary lifestyle and cardiovascular outcomes in Korean population are warranted to confirm the present results.