Preventing a Mass Disease: The Case of Gallstones Disease: Role and Competence for Family Physicians
Article information
Abstract
Gallstone formation is the result of a complex interaction between genetic and nongenetic factors. We searched and reviewed the available literature to define how the primary prevention of gallstones (cholesterol gallstones in particular) could be applied in general practice. Electronic bibliographical databases were searched. Prospective and retrospective cohort studies and case–controlled studies were analyzed and graded for evidence quality. The epidemiological data confirmed that genetic factors are estimated to account for only approximately 25% of the overall risk of gallstones, while metabolic/environmental factors are at least partially modifiable in stone-free risk groups, and are thus modifiable by primary prevention measures related to diet, lifestyle, and environmental factors (i.e., rapid weight loss, bariatric surgery, somatostatin or analogues therapy, transient gallbladder stasis, and hormone therapy). There is no specific recommendation for the secondary prevention of recurrent gallstones. Family physicians can contribute to preventing gallstones due to their capability to identify and effectively manage several risk factors discussed in this study. Although further studies are needed to better elucidate the involvement of epigenetic factors that may regulate the effect of environment and lifestyle on gene expression in the primary prevention of gallstone formation, preventive interventions are feasible and advisable in the general practice setting.
INTRODUCTION
Gallstone disease (GSD) is one of the most frequent gastro-intestinal disorders in westernized countries,123) including Europe.4) There are 3 types of gallstones that develop in the gallbladder and bile ducts, and they are distinguished by their chemical composition: pure cholesterol, pure pigment, or mixed (containing small amounts of bilirubin salts and calcium). In industrialized countries, 75% of gallstones are composed of cholesterol, approximately 20% are black pigment stones and 5% are brown pigment stones (Figure 1).5678) The costs associated with disease management are high because of the diagnostic and surgical procedures involved.9) Owing to the interplay of metabolic and lifestyle factors in the pathogenesis of GSD,210) family physicians (FPs) may play an important role in the prevention of GSD by providing patients with education.
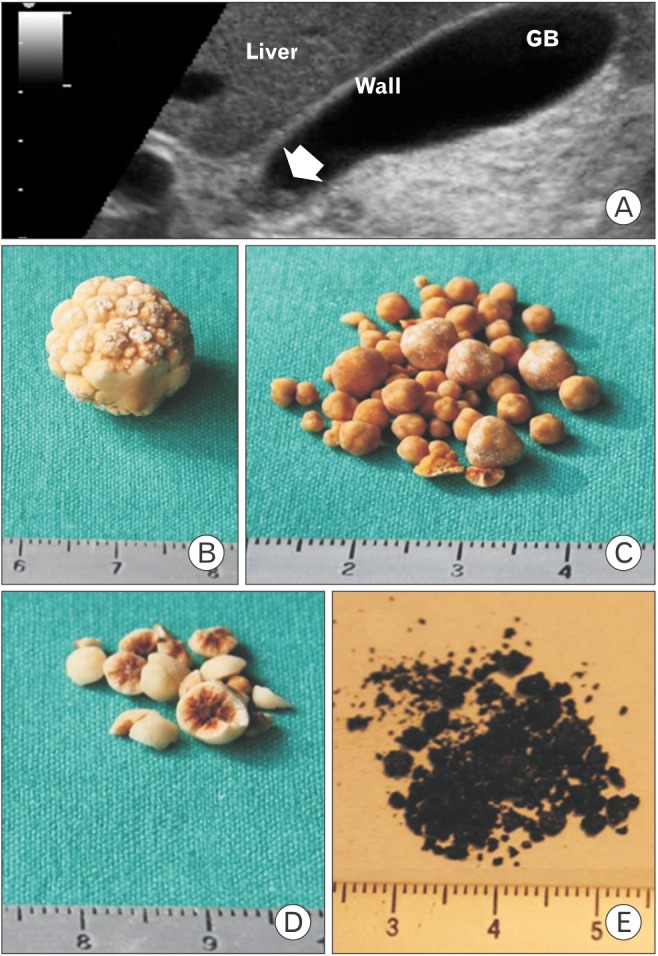
The burden of gallstone disease. (A) Ultrasonographic appearance of a single small gallstone (0.4 mm) within the GB neck (arrow), seen on a longitudinal transabdominal scan. The hyperechogenic spot is mobile, with decubitus, and is not associated with a posterior acoustic shadow. The GB wall is not thickened (i.e., ≤3 mm in the fasting state) and the remaining lumen is anechoic. A 1-cm scale is shown on the left. (B) Macroscopic appearance of a solitary pure cholesterol gallstone (approximately 12 mm) showing yellowish morular surfaces. (C) Multiple cholesterol gallstones (2–5 mm) with smooth surfaces. (D) Multiple mixed cholesterol gallstones (approximately 5 mm) with pigment centers on the cut surfaces. (E) Multiple black pigment gallstones, forming a largely friable sandy powder (approximately 1 mm). GB, gallbladder.
In this review, we aimed to identify the essential issues related to the prevention of GSD and to provide FPs with the most current and relevant information for use in their daily clinical practice.
SEARCH METHODOLOGY
We assessed all literature published from 1974–2015 by searching PubMed (http://www.ncbi.nlm.nih.gov/pubmed). Keywords included the terms 'bile acids,' 'biliary stones,' 'choledocholithiasis,' 'gallbladder,' 'gallstones,' 'prevention,' 'obesity,' 'metabolic syndrome,' 'bariatric surgery,' 'very low-calorie diet,' and 'ursodeoxycholic acid or cholesterollowering drugs,' Prospective, retrospective cohort studies, case–controlled studies, and meta-analyses published in the English language in peer-reviewed international journals with adequate impact factors were analyzed. Final selection was based on whether the papers were relevant to clinical practice.
MAIN MESSAGES: THE ESSENTIAL QUESTIONS AND ANSWERS
1. Who Are the Subjects at Risk of GSD, and What Are the Most Common Modifiable Factors Involved in the Prevention of GSD?
Several pathogenic mechanisms have been linked to cholesterol GSD, namely genetic predisposition influencing cholesterol homeostasis (and possibly epigenetic changes), hepatic hypersecretion of cholesterol leading to supersaturated bile, and accelerated precipitation of solid cholesterol crystals in a hypomotile gallbladder, accommodating more mucins. Increased absorption of cholesterol from the intestine is another factor.2) Although a family history of the disease is often suggestive of the role of genetic factors,11) genes are estimated to account for only approximately 25% of the overall gallstone risk, as suggested by the analysis of the Swedish twin registry.12) In the majority of cases, a genetic background that involves multiple pathways13) determines an individual's predisposition to developing cholesterol gallstones in response to a number of acquired unmodifiable and modifiable environmental factors (Table 1).14) As with other chronic metabolic diseases, GSD is affected by gene-environment interactions and gene expression that is possibly regulated by epigenetic mechanisms.14) Preventive measures are especially effective against cholesterol gallstones because modifiable pathogenic factors are often involved.
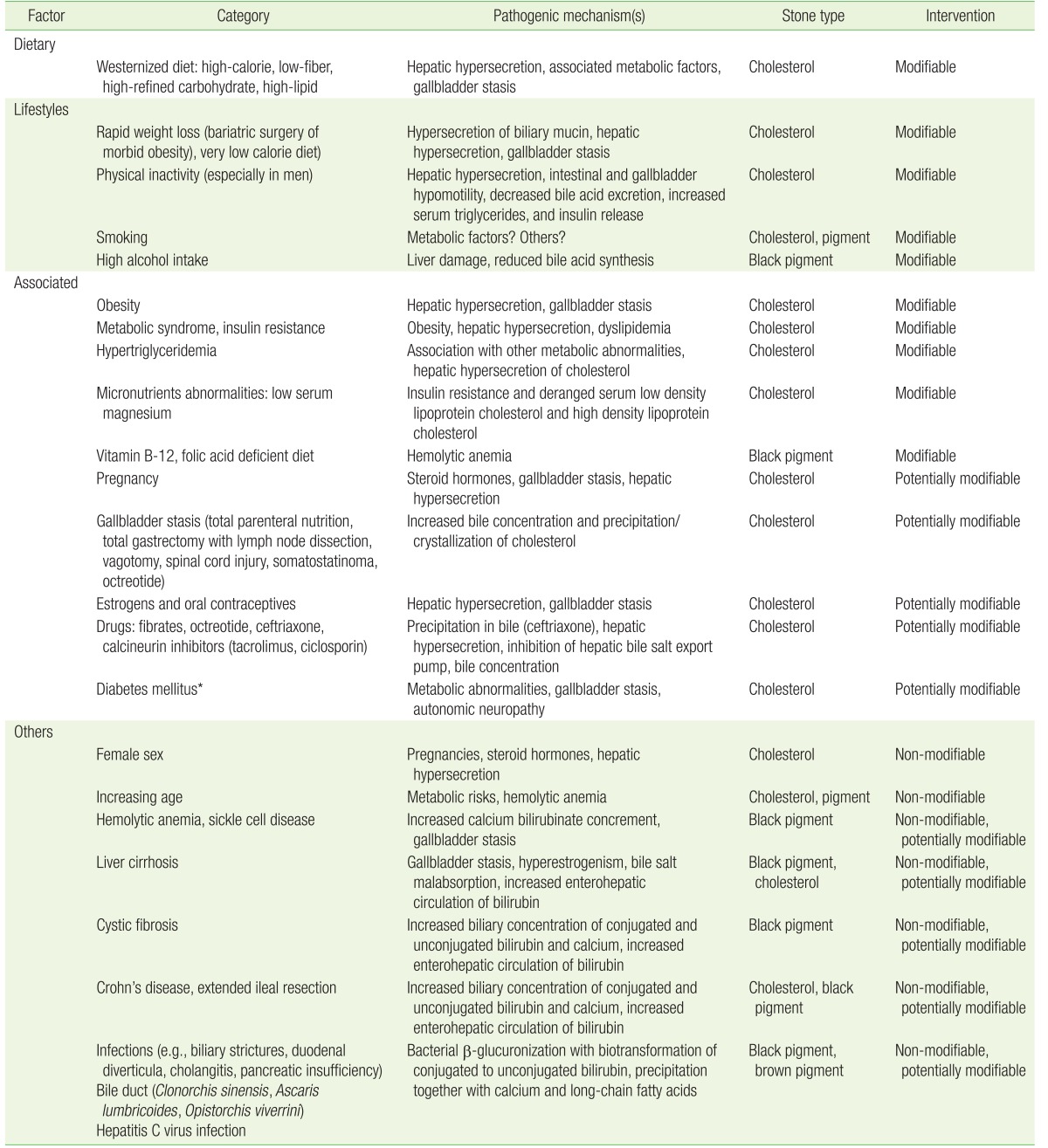
Non-genetic risk factors for gallbladder stones including modifiable, potentially modifiable, and non-modifiable factors
1) Obesity and metabolic factors
The main risk factors for cholesterol gallstones (e.g., obesity, type-2 diabetes, dyslipidemia, and hyperinsulinemia) are the components of metabolic syndrome.2) Increased body mass index is a risk factor for gallstone formation and growth2) and acts as an independent risk factor for symptomatic GSD, particularly in women.15) Waist circumference and triglyceridemia are correlated with GSD.16) Additional obesity-related pro-lithogenic factors include gallbladder stasis,17) insulin resistance, and reduced high density lipoprotein (HDL)-cholesterol.16) Appropriate lifestyle interventions may influence the pathogenesis of cholesterol gallstones, and should focus on maintaining an ideal weight in people with normal weight and weight loss in overweight and obese individuals.15) The key mechanisms regulating this pathogenic process seem to involve gene-environment interactions through epigenetic mechanisms that also occur during the fetal stage and involve factors such as lifestyle, toxic agents, and environmental pollutants.18)
2) Physical activity
People should be aware of the importance of performing regular physical activity whenever possible.19) The overall beneficial effect of exercise goes beyond simple protection against gallstone formation.20) In the Epic-Norfolk prospective cohort study, energy expenditure and cardio-respiratory fitness21) were investigated via questionnaires in 25,639 volunteers (range, 40 to 74 years old). Subjects were monitored over 14 years. After 5 years, 135 cases of symptomatic gallstones (70% women, 69% uncomplicated) were observed. After 14 years, 290 cases of symptomatic gallstones (68% women, 54% complicated) were recorded. The highest level of physical activity was associated with a 70% decreased risk of symptomatic gallstones in both sexes, with a likely causal effect seen after 5 years. Hyperinsulinemia promotes the hepatic uptake of cholesterol,22) with increased secretion in bile23) and decreased secretion of bile acids24) (leading to supersaturated lithogenic bile). Regular exercise reduces insulin levels,25) insulin resistance,26) triglyceridemia, 27) and fatty acid-dependent hypersecretion of gallbladder mucin,28) and increases serum HDL-cholesterol.29) HDL-cholesterol is the precursor of bile acids30) and is inversely related to gallstone prevalence.31) Finally, physical activity promotes cholecystokinin-dependent gallbladder contraction.32)
3) Dietetic factors
Long-term population-based prospective studies have highlighted difficulties in estimating the quantity and ingestion patterns of nutrients. High-fiber and high-calcium diets reduce biliary hydrophobic bile acids, while a regular eating pattern decreases gallbladder stasis by promoting regular emptying.19) Both aspects play a preventive role against GSD. The likelihood of GSD is increased by westernized diets, including meat intake.33) Fruit and vegetables34) might be protective against GSD, but the data remain controversial. Unsaturated fats35) might protect against GSD. Coffee has been reported to be protective in some,3637) but not all, epidemiological studies.38) Although prospective epidemiological studies reported protective effects of alcohol consumption on gallstone formation,16) and a Danish Mendelian randomization study indicated that patients with symptomatic gallstones consumed less alcohol compared to those with asymptomatic stones,15) the findings are controversial,39) and alcohol consumption cannot be recommended for the prevention of gallstones. Vitamin C supplementation may have a protective effect against GSD. Cholesterol conversion to bile acids requires 7α-hydroxylation and appropriate hepatocyte content of vitamin C.40) Vitamin C deficiency might therefore increase the risk of cholesterol gallstone formation.41) Vitamin C supplementation (500 mg, 4 times/d) was shown to change biliary bile acid composition, increase phospholipids, and prolong the cholesterol crystallization time.42) Observational studies have identified an association between low vitamin C consumption and GSD risk.41) In the EMIL observational population-based study (n=2,129 subjects; range, 18 to 65 years old), gallstone prevalence was 4.7% vs. 8.2% in patients reporting regular use of vitamin C (n=232) compared to those who did not report using vitamin C regularly (n=1,897).43)
2. How to Screen People at Risk?
Abdominal ultrasonography is the most convenient first-line screening test because of its non-invasiveness, low costs, simplicity, and high sensitivity and specificity for detecting the presence of gallstones (84% and 99%, respectively).44) The same procedure allows a detailed and simultaneous study of gallbladder morphology (wall thickness, presence of polyps, sludge) and kinetics (fasting and postprandial gallbladder volume with estimation of half-emptying time in response to a standard fatty meal.217) Compared to ultrasonography, computed tomography (CT) does not show gallstones if the concretion is isodense with bile.45) CT with quantitative assessment of stone density may help to select patients for oral bile acid litholysis (i.e., presence of small [<5 mm], uncalcified [radiotransparent] gallstones).46) For choledocholithiasis, magnetic resonance cholangiopancreatography is the first choice approach because it is noninvasive and has high sensitivity and specificity compared to ultrasonography.47) Endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography have high sensitivity (range, 80% to 90%) and specificity (100%), but are invasive.47) Furthermore, neither method is free of complications.
3. Is Any Form of Pharmacological Prevention of Gallstones Effective in the General Population?
No rationale exists for using pharmacological therapy for preventing GSD. The studies published so far were mainly experimental or incomplete, with a lack of clinical relevance. The investigated agents include the bile acid ursodeoxycholic acid (UDCA), omega-3 fatty acids,48) statins,18) ezetimibe,184950) aspirin,51) and liver nuclear receptor regulators of cholesterol metabolism, i.e., FXR (farnesoid X receptor) agonists.2)
4. Are There Specific Subgroups of Subjects in Which Primary Prevention Is Feasible and Sustainable?
Approaches to primary and sometime secondary preventive measures are especially effective in the case of cholesterol gallstones (Figure 2).
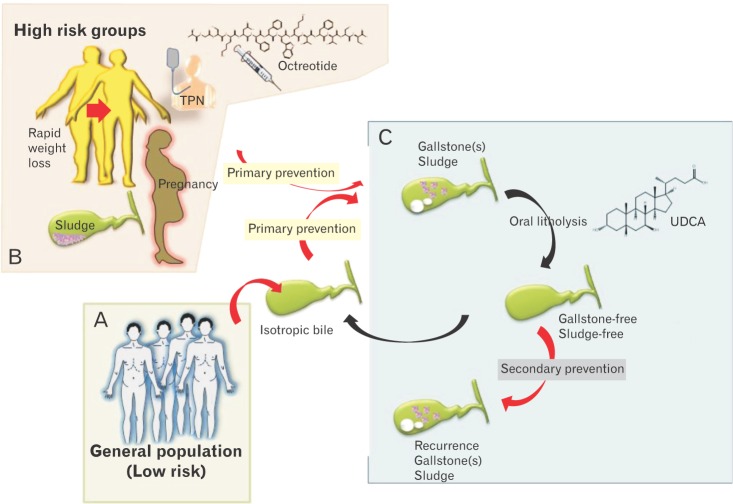
Preventive measures are especially effective in the case of cholesterol gallstones. (A) Primary prevention of gallstones (which contributes to maintaining isotropic bile, meaning free of cholesterol crystals and stones), is already indicated in the general population (at low risk) by generally maintaining healthy lifestyles. (B) Tailored forms of prevention are indicated particularly in high-risk groups (see text and Table 2). Patients with known biliary sludge, pregnant women, patients undergoing rapid weight loss, patients on long-term octreotide, and those receiving long-term total parenteral nutrition are at the highest risk of developing gallstones and subsequent biliary symptoms and/or gallstone-related complications. Once gallstones/sludge are formed, oral litholysis (by ursodeoxycholic acid) has a very limited role in a small subgroup of symptomatic patients with small, pure cholesterol stones in a functioning gallbladder. (C) If dissolution of concrements is achieved, secondary prevention is indicated in the subgroup of patients at risk of recurrent gallstones/sludge. TPN, total parenteral nutrition; UDCA, ursodeoxycholic acid.
1) Obese patients undergoing rapid weight loss
If weight loss is rapid (i.e., over 1.5 kg/wk),52) the risk of gallstones increases significantly, although they tend to be asymptomatic in such cases. This is the case in patients starting very-low-calorie diets (i.e., <800 kcal/d)53) or undergoing bariatric surgery (up to 48% of patients for weight loss exceeding 25% of their original weight).5354) The overall risk decreases when body weight stabilizes after approximately 24 months.53) Weight cycling also represents an independent risk factor for gallstones.55) Excessive de novo biosynthesis of cholesterol and biliary cholesterol excretion are the two main pathogenic factors.56) Some preventive measures are possible during weight-reducing programs.
It is advisable to keep the rate of weight loss to <1.5 kg/wk.5257) The risk of developing symptomatic gallstones decreases if gallbladder motility is improved by appropriate fat content in the diet (at least 7 g/d).53) UDCA, which is litholytic and hydrophilic, greatly decreases the risk of cholesterol gallstone formation (<10%) and of gallstones becoming symptomatic,58) following rapid weight loss.5859) A meta-analysis of 5 randomized controlled trials including 521 patients (322 taking UDCA and 199 taking a placebo) concluded that UDCA 300–1,200 mg/d effectively prevents gallstone formation after bariatric surgery,59) reducing the incidence from 32% to 2%,60) with no severe side effects. The beneficial effect of (n-3) polyunsaturated fatty acids (11.3 g/d) on biliary cholesterol nucleation time and crystallization and the prevention of gallstone formation was confirmed in a randomized, doubleblind placebo-UDCA (1,200 mg/d)-controlled trial in obese women on hypocaloric diets (1,200 kcal/d, 20% energy from fat).48) The protective mechanism is probably mediated by the replacement of biliary arachidonate by (n-3) polyunsaturated fatty acids,61) increasing biliary phospholipids,62) and changing intrahepatic cholesterol transportation and the hypersecretion of biliary cholesterol.63) Concurrent prophylactic cholecystectomy has previously been recommended based on the assumption that almost 19% of patients might require a cholecystectomy following bariatric surgery.64) The data on this are inconclusive, since up to 97% of patients remain asymptomatic as confirmed by a recent decision analysis model.65)
2) Patients on long-term therapy with somatostatin or analogues
These patients exhibit biliary lithogenic changes and gastrointestinal motility changes, including delayed intestinal transit and gallbladder stasis.6667) Prophylactic therapy with UDCA has been suggested for these patients.676869)
3) Patients with marked gallbladder stasis
Gallbladder stasis and changes in biliary composition are typical in pregnancy70) or during prolonged fasting such as during total parenteral nutrition (TPN). Both sludge and small gallstones might disappear spontaneously in the postpartum period70) and when the oral diet is resumed following TPN.71) Therefore, there is no indication for oral litholysis in either of these conditions.
4) Patients on hormone therapy
A metanalysis72) showed a significantly increased risk of GSD in women under hormone replacement therapy for the control of menopause symptoms or the prevention of osteoporosis.73) The possibility of any pharmacological preventive approach has not been addressed, and therefore has no rationale as yet.
5. Are There Any Recommendations for the (Secondary) Prevention of Recurrent Gallstones?
1) Recurrent gallstones
The dissolution rate of cholesterol gallstones is 37% to 60%74) after 2 years of treatment with UDCA. Recurrence is high following dissolution (15% by 1 year and 45% by 5 years).757677) The pharmacological prophylaxis of gallstone recurrence should be restricted to very high-risk subgroups or to patients not fitting the criteria of subsequent cholecystectomy.
2) Recurrent bile duct stones
There are no evidence-based prophylactic measures able to prevent the recurrence of bile duct stones.
3) Patients with low phospholipid-associated cholelithiasis
Heterozygous mutation of the gene 'ABCB4,' encoding the phospholipid-flippase, is a rare form of monogenic predisposition for cholelithiasis associated with low biliary phospholipids and bile salt-mediated damage of the canalicular membrane. In patients with this mutation, gallstones, intrahepatic sludge, and microlithiasis develop before the age of 40, while biliary symptoms recur after cholecystectomy.7879) A few studies have suggested that long-term prophylactic therapy with UDCA should be initiated as early as possible.7879)
CONCLUSION
The epidemiology of GSD (including complications) and the costs associated with its management make all possible primary prevention strategies worthwhile. In general practice, attention should be paid to identifying general and specific modifiable risk factors for GSD and subgroups of patients at risk of GSD. In this setting, educational intervention aiming to prevent GSD should focus on helping patients to have healthy lifestyles, maintain their ideal body weight, partake in regular physical activity, prevent metabolic syndrome, and control all factors influencing glycolipid metabolism and ultimately biliary cholesterol saturation. Pharmacological interventions should be restricted to certain subgroups of patients (Table 2). Further studies will be needed to address the involvement of epigenetic factors regulating gene expression in response to environmental factors in order to identify even better preventive measures.
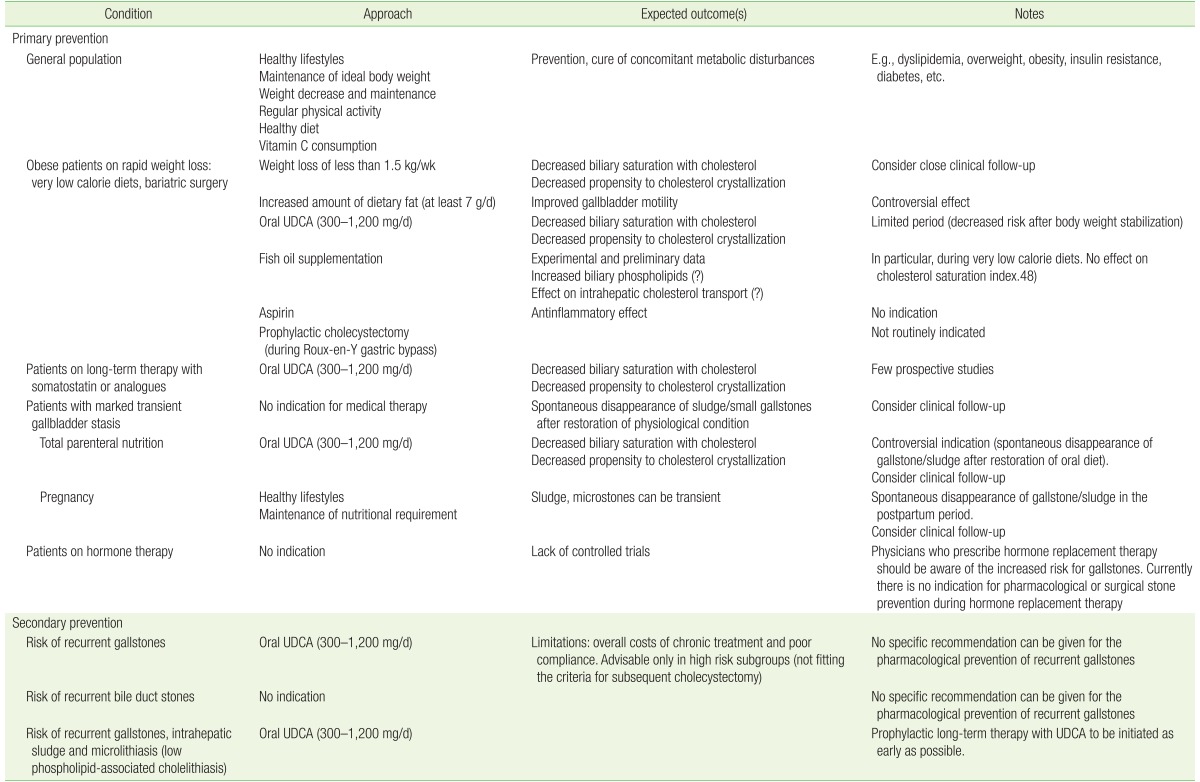
Current status of preventive approaches to cholesterol GSD
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.