INTRODUCTION
Liver fibrosis resulting from chronic liver injury progressively evolves into liver cirrhosis, which is a major cause of mortality worldwide [1]. The primary causes of liver fibrosis are viral infections (hepatitis B and C), alcohol abuse, non-alcoholic steatohepatitis, autoimmune hepatitis, and systemic diseases [2,3]. Recent studies have suggested that reproductive factors, including hormone therapy and menopause, may also be risk factors for liver fibrosis [4-11]. However, the association between a history of pregnancy, which is an important reproductive factor, and liver fibrosis remains unclear.
To the best of our knowledge, only two previous studies have investigated the association between pregnancy and liver fibrosis in women infected with hepatitis C virus and have reported inconsistent results. Furthermore, data on the association between a history of pregnancy and liver fibrosis in the general population are limited.
Methods for assessing liver fibrosis include liver biopsy, transient elastography, magnetic resonance elastography, and non-invasive scores [12]. Non-invasive and inexpensive methods may be feasible in general population settings. The Fibrosis-4 index (FIB-4) has been validated as a surrogate marker of advanced fibrosis (bridging fibrosis or cirrhosis) and is suggested to be superior to multiple non-invasive markers of liver fibrosis [13,14].
Therefore, this nationwide, population-based study aimed to elucidate the association between a history of pregnancy and liver fibrosis using FIB-4 in postmenopausal Korean women. We further investigated the association between liver fibrosis and other female reproductive factors, including total reproductive years, age at menarche and menopause, and the use of oral contraceptives.
METHODS
1. Data Source
This study was based on data from the Korea National Health and Nutrition Examination Survey (KNHANES) conducted in South Korea since 1998 by the Division of Chronic Disease Surveillance of the Korea Centers for Disease Control and Prevention (currently Korea Disease Control and Prevention Agency) and the Korean Ministry of Health and Welfare. This population-based, cross-sectional survey included a nationally representative sample of the non-institutionalized civilian population selected via a complex, stratified, multistage, probability-cluster rolling sampling design to assess the nutritional and health status of the Korean population. The survey consisted of health interviews, health examinations, and nutrition questionnaires for individuals in Korea. The study was conducted in accordance with the Declaration of Helsinki. Before the survey was performed, all participants were provided with information regarding the survey, and written consent was obtained from each participant.
2. Study Population
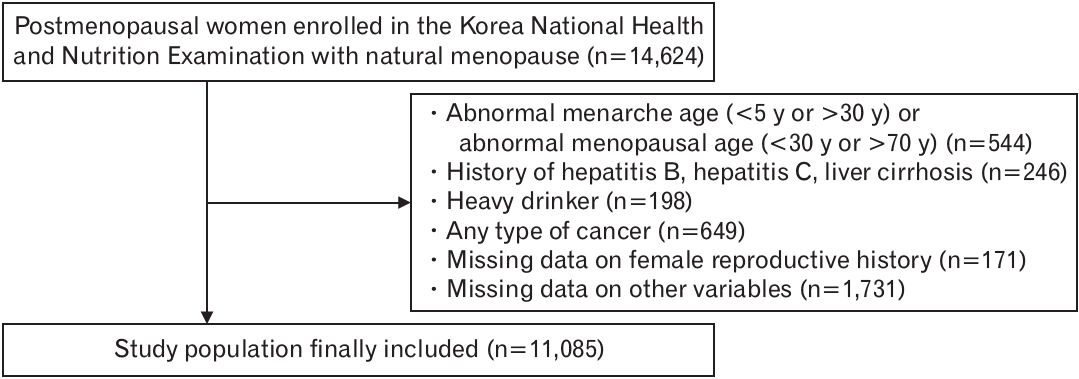
This study analyzed the KNHANES data obtained from a representative sample between 2008 and 2017, including surveys from the second and third years of KNHANES IV (2008–2009), V (2010–2012), VI (2013–2015), and VII (2015–2017). The study population included postmenopausal women who completed the health examination survey, which included their entire female reproductive history. Among 46,365 women who participated in the 2008–2017 KNHANES, 14,624 women with natural menopause were initially selected. Women with extremely early menarche (age <5 years) or extremely late menopause (age >70 years) were excluded (n=544). In addition, participants with hepatitis B, hepatitis C, liver cirrhosis (n=246), heavy alcohol consumption (>140 g/wk) (n=198), or cancer (n=649) were excluded. After excluding those with missing values for any other variables (n=171), 11,085 women were finally selected (Figure 1).
3. Definition of Liver Fibrosis
The risk of liver fibrosis was assessed using the following non-invasive equation: FIB-4=age (years)×aspartate aminotransferase (AST, IU/L)/[platelet count (109/L)×√alanine aminotransferase (ALT, IU/L)].
A previously published cutoff was used to exclude and diagnose advanced liver fibrosis. FIB-4 score ≥2.67 is considered a high-risk cutoff for advanced liver fibrosis in women with a high predictive value [13,15]. In addition, FIB-4 has proven to be useful in detecting liver fibrosis in Korea [16]. In addition, many studies on liver fibrosis in Korea have been successfully conducted using FIB-4 [17-22].
4. Covariates
The participants in the KNHANES were asked about their demographic, social, lifestyle, and medical conditions, including age, education, urban residence, alcohol or cigarette use, and household income. The participants were classified on the basis of education, based on the highest degree of educational attainment, into those who attained high school or higher degrees (highly educated group=yes). They were further classified based on their monthly household income into quartiles, and those in the lowest quartile were identified as the lower-income group. Regarding alcohol consumption, participants who consumed alcohol at least once a month were categorized as “alcohol consumption=yes.” As for smoking status, participants were categorized into two groups according to whether they were currently smoking at the time of the survey. Participants living in an urban residence were defined as those whose residential area was the “dong,” which implies a Korean urban address. Participants with a history of certain comorbidities were those who provided a “yes” response to the question about the diagnosis of certain diseases, including type 2 diabetes, hypertension, dyslipidemia, cardiovascular disease, chronic kidney disease, stroke, and thyroid disease.
5. Statistical Analysis
Data from KNHANES were obtained from a sample of the Korean population; hence, the analysis required that sampling weights be included to calculate the estimate, taking into consideration the representativeness of the Korean population. P-values were calculated using a two-sample t-test for continuous variables. The chi-square test was used to analyze categorical variables. Multivariate-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using multiple logistic regression analyses to evaluate the association of the number of pregnancies and other female reproductive factors with liver fibrosis.
The entire population was grouped into quartiles according to the number of pregnancies, total reproductive years, age at menopause, and age at menarche, and the P-values for linear trends of liver fibrosis across the variables were calculated. Pre-specified subgroup analyses were performed, and P-values for interaction according to each covariate were reported. All statistical analyses in this study were performed using the SAS ver. 9.3 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at P<0.05.
RESULTS
1. Baseline Characteristics
The baseline characteristics of the study population are presented in Table 1. Participants with liver fibrosis were older (P<0.001), drank less alcohol (P=0.011), had lower levels of education (P<0.0001), had lower income (P<0.001), weighed lesser (P<0.001), and were shorter (P<0.001) than those without liver fibrosis.
Individuals with liver fibrosis had a higher prevalence of hypertension (P=0.001), cardiovascular disease (P=0.001), and stroke (P=0.003) than those without liver fibrosis. Furthermore, individuals with liver fibrosis had higher systolic blood pressure (P<0.001), higher diastolic blood pressure (P=0.002), lower cholesterol levels (P<0.001), lower triglyceride levels (P=0.0003), higher AST levels (P<0.001), higher ALT levels (P<0.001), higher creatinine levels (P=0.015), and lower triglyceride levels (P<0.001) than those without liver fibrosis.
Regarding reproductive factors, individuals with liver fibrosis were older at menarche (P=0.003), had shorter total reproductive years (P=0.004), and had fewer pregnancies (P=0.0003) than those without liver fibrosis. The use of oral contraceptives showed no statistically significant difference between the two groups.
2. Association of History of Pregnancy and Other Reproductive Factors with Risk of Liver Fibrosis
Participants who had never been pregnant had a higher risk of liver fibrosis than those who had a history of one or more pregnancies (adjusted OR, 0.30; 95% CI, 0.15–0.59) (Table 2). Furthermore, participants with one pregnancy (adjusted OR, 0.15; 95% CI, 0.04–0.51), two pregnancies (adjusted OR, 0.32; 95% CI, 0.14–0.73), and three or more pregnancies (adjusted OR, 0.30; 95% CI, 0.15–0.6) had lower risks of liver fibrosis than those who had never been pregnant (model 4, Table 2). In individuals who had experienced one or more pregnancies, a higher number of pregnancies was not associated with liver fibrosis after adjusting for age, obesity, income level, education level, alcohol consumption, smoking status, urban residence, type 2 diabetes, hypertension, dyslipidemia, cardiovascular disease, chronic kidney disease, stroke, or thyroid disease (P=0.135) (Table 2). Furthermore, other female reproductive factors, including total reproductive years, age at menopause and menarche, and use of oral contraceptives, showed no statistically significant association with the risk of liver fibrosis.
3. Subgroup Analysis
We performed stratified subgroup analyses according to education level, lower income, alcohol consumption, current smoking status, urban residence, type 2 diabetes, hypertension, dyslipidemia, obesity, stroke, cardiovascular disease, chronic kidney disease, and thyroid disease (Table 3). The association between history of pregnancy experience and liver fibrosis did not differ according to the subgroups (P for interactions: education, 0.788; lower income, 0.329; alcohol consumption, 0.775; urban residence, 0.374; hypertension, 0.451; type 2 diabetes, 0.27; dyslipidemia, 0.554; obesity, 0.49; stroke, 0.9; and cardiovascular disease, 0.698). Subgroup analysis of the current smoking status, chronic kidney disease, and thyroid disease could not be performed as none of the participants reported having these conditions.
DISCUSSION
This nationally representative population-based study demonstrated that postmenopausal women with a history of pregnancy had a reduced risk of liver fibrosis. Among those that had been pregnant, the number of pregnancies was not associated with the risk of liver fibrosis. To the best of our knowledge, this is the first study to report an association between a history of pregnancy and liver fibrosis in postmenopausal women.
Two studies have previously investigated the association between pregnancy and liver fibrosis in women with hepatitis C; however, these reported inconclusive results [5,23]. One study concluded that the long-term impact of pregnancy on hepatitis C virus (HCV)-related histological lesions is potentially protective against fibrosis progression [5]. Another study suggested that pathological exacerbation, including liver fibrosis, could occur following delivery in women with HCV infection [23]. To date, no study has yet reported an association between pregnancy and liver fibrosis in the general population.
In this study, 3.3% of the participants were at high risk of developing advanced liver fibrosis (bridging fibrosis or cirrhosis). A recent study included individuals who underwent health checkups at 13 health promotion centers in Korea between 2018 and 2020, and the prevalence of advanced liver fibrosis was 2.6% [24]. Another study reported that the FIB-4 index produced a predictive rate of liver fibrosis similar to the magnetic resonance elastography method [25].
Several studies have reported that a lack of estrogen may be an independent risk factor for liver fibrosis [6,26,27]. Compelling evidence exists regarding the protective role of estrogen against liver fibrosis via its reduction effects on hepatic mRNA for type I and III procollagens, and the tissue inhibitor of metalloproteinase 1, as well as on the deposition of types I and III collagen protein, total hepatic collagen, and malondialdehyde, which is a product of lipid peroxidation [28]. Maternal excretion of estrogen during the gestational period increases up to approximately 100-fold and its serum concentration increases by 10-fold [29-31]. A high estrogen surge during pregnancy may play a protective role against liver fibrosis. In addition, the amount of estrogen during the gestational period is much higher than the amount excreted during the entire non-pregnancy period. These findings indicate that sufficient endogenous estrogen exposure in women with a history of pregnancy may prevent the development of liver fibrosis during the postmenopausal period. Further studies are needed to elucidate the other mechanisms underlying the association between pregnancy and liver fibrosis.
Our study had several strengths. First, this was the first study to demonstrate an association between a history of pregnancy and liver fibrosis in the general population. Second, this was a large-scale, nationwide study that used stratified, multistage probability sampling data, and sampling weights for the analysis. The results of our study can therefore be generalized to the entire Korean population. Third, we adjusted the data for multiple confounding variables including income level, education level, urban residence, alcohol consumption, smoking status, and major comorbidities.
This study had some limitations. First, the FIB-4 index is not the gold standard for detecting liver fibrosis, and a liver biopsy is necessary for a precise diagnosis of liver fibrosis. However, in the general population, non-invasive diagnostic methods, including the FIB-4 score, have been widely applied while considering the complications and costs. The FIB-4 score is reliable for diagnosing liver fibrosis [13], has been validated in several studies on the etiologies of liver disease, and has been shown to be superior to other non-invasive markers of liver fibrosis [32,33]. Second, recall bias might have existed. Age at menopause or menarche was not analyzed based on the responses to the questionnaires. Third, we did not perform a subgroup analysis on the participants’ current smoking status, chronic kidney disease, and thyroid disease status because no relevant data were reported for the subgroup analysis.
In conclusion, we reported that a history of pregnancy was associated with a reduced risk of liver fibrosis in postmenopausal women. Our findings indicate a protective role of pregnancy against liver fibrosis in postmenopausal women. Therefore, women who have never been pregnant should be aware of the risk of liver fibrosis and the need for early prevention.