Association Between the Awareness of Dyslipidemia and Health Behavior for Control of Lipid Levels Among Korean Adults with Dyslipidemia
Article information
Abstract
Background
Dyslipidemia is a major risk factor contributing to cardiovascular disease and its prevalence is steadily rising. Although screening tests are readily accessible, dyslipidemia remains undertreated. Evaluating health behavior patterns after diagnosis may help improve lifestyle interventions for the management of dyslipidemia.
Methods
Data from the fifth Korean National Health and Nutrition Examination Survey 2010–2012 were used. A total of 6,624 dyslipidemia patients over 20 years old were included according to National Cholesterol Education Program-Adult Treatment Panel III guidelines. Logistic regression analysis was completed using a weighted method to determine whether awareness of dyslipidemia was associated with health behavior. Health behavior was divided into two categories: behavioral factors (smoking, alcohol consumption, exercise) and nutritional factors (adequate intake of fiber, carbohydrate, fat, protein).
Results
There were no significant differences in health behavior among dyslipidemia patients according to awareness after adjustment for covariates, diabetes and hypertension. Awareness in women was associated with decreased smoking (odds ratio [OR], 0.55; 95% confidence interval [CI], 0.32 to 0.94), but when adjusted for diabetes and hypertension the result was not significant (OR, 0.61; 95% CI, 0.35 to 1.06). The same pattern applied to intake of carbohydrate in men (OR, 1.28; 95% CI, 0.99 to 1.67) and protein in women (OR, 1.22; 95% CI, 0.98 to 1.50). In subgroup analysis, awareness of dyslipidemia in men without hypertension or diabetes was associated with adequate intake of carbohydrate (OR, 1.70; 95% CI, 1.06 to 2.72).
Conclusion
Increasing awareness alone may not be enough to improve healthy behavior in patients with dyslipidemia. Efforts including patient education and counseling through a multi-team approach may be required.
Introduction
Cardiovascular disease (CVD) is one of the main causes of morbidity and mortality worldwide.1) According to 2013 death statistics in Korea, CVD was the second leading cause of death.2) Previous studies have declared that dyslipidemia is an important risk factor for CVD by contributing to the initiation and progression of atherosclerosis; therefore, its management is important for reducing the burden of CVD.3)
Meanwhile, the prevalence of dyslipidemia is steadily rising in Korea, and statistics published by the Korean Society of Lipidology and Atherosclerosis (KSLA) revealed that in 2013 57.6% of men and 38.3% of women, accounting for a total of 47.8% of people over 30 years of age (more than 16 million), had dyslipidemia. When the low-density lipoprotein cholesterol (LDLC) cutoff value was set to 100 mg/dL for diabetic patients, 9 out of every 10 diabetic adults had dyslipidemia. For patients with hypertension, 2 out of every 3 hypertensive adults were diagnosed with dyslipidemia.4)
The use of lipid-lowering medications such as statin and fibrate are important for the treatment of dyslipidemia, especially in high-risk patients. However, lifestyle interventions are also important for managing dyslipidemia and are considered initially after diagnosis, since dietary factors can influence lipid levels and regular exercise improves lipid profiles, while smoking has been known to have a detrimental effect.5) Villegas et al.6) reported that a combination of protective factors including normal body mass index (BMI), never smoking, light alcohol consumption, prudent diet and regular physical activity was associated with a significantly lower prevalence of dyslipidemia. Pharmacological therapy requires diagnosis by a doctor, and patients may be initially reluctant to take daily medication, making lifestyle interventions an attractive first choice for intervention. In fact, patients may be more compliant to behavioral modification and behavioral factors have the advantage that intervention for prevention of chronic diseases and lowering of cardiovascular risks can be emphasized at the population level. The Nurses' Health Study cohort was able to conclude that adherence to lifestyle guidelines for diet, exercise, and smoking was associated with a very low risk for coronary heart disease.7)
Previous reports have studied the prevalence, awareness, and treatment of dyslipidemia in Korea. Although awareness and treatment rates are slowly rising, their rates are still low (13.7% and 7.4% in 2010 compared to 6.1% and 1.9% in 2005, respectively).8) As for lifestyle interventions, there is a lack of studies examining adherence rates to clinical guidelines for lifestyle therapy in those with dyslipidemia, especially comparing those who are aware and those who are not aware of their diagnosis.
Lack of awareness about dyslipidemia may act as an additional barrier to adequate health behavior. However, whether awareness of dyslipidemia affects health behavior is not clear. In a study by Kitagawa et al., patients with high awareness of their health status showed a positive attitude towards diet and exercise as lipid-lowering treatment, and high adherence to drug therapy. However, subjects were limited to high-risk patients on prescription for pravastatin making it difficult to apply the results to the general population.9) Another study conducted in a Chinese province that analyzed dyslipidemia awareness and influencing factors demonstrated that awareness was associated with a lower odds ratio (OR) for drinking (OR=0.78) and physical activity (OR=0.714), and with higher OR for increased BMI (OR=1.547), age (increasing OR for older age groups), education (higher OR for higher level of education), and family history of dyslipidemia (OR=3.62).10) However, criteria for the factors mentioned were looser than clinical guidelines: drinking any kind of alcohol more than once a week, obesity as BMI ≥24 kg/m2, and exercising not less than once a week.
No other studies analyzing awareness of dyslipidemia and associated factors were found by the authors. Therefore, this study compared adherence to health behavior according to clinical guidelines between dyslipidemia subjects who were aware of their diagnosis and those who were not, with higher adherence expected in the awareness group.
Methods
1. Study Population
This study was performed using data from the fifth Korean National Health and Nutrition Survey 2010–2012 (KNHANES V). The KNHANES is a nationally representative study conducted regularly by the Korea Centers for Disease Control and Prevention to assess the health and nutritional status of non-institutionalized civilians in Korea. It uses a multi-stage probability sample design and trained interviewers to administer questionnaires to participants. The KNHANES V is based on data from 3,800 households in 576 randomly selected survey areas, with the number selected in proportion to the size of each area.11) For the selection of dyslipidemia patients, from a total of 25,334 individuals that participated in the KNHANES V, we excluded those aged <20 years (n=6,140), those who did not provide an answer for the assessment of awareness of dyslipidemia (n=1,518), whose lipid profiles were not assessed (n=959), and those who did not fast for over 9 hours (n=485). Those without available data for adequate physical activity, BMI, self-perceived health status, education, household income, and nutrient intake (n=2,115) were also excluded in the final analysis. The present study received an exemption from informed consent by the institutional review board committee of the Seoul National University Hospital because this study used public data provided by the KNHANES (IRB No. X-1602-333-903).
2. Measurement
Blood samples were collected from each participant the morning after fasting for at least 8 hours. Samples were processed, refrigerated immediately, and transported to the central laboratory to be analyzed within 24 hours after transportation. Total cholesterol (TC), high-density lipoprotein cholesterol (HDLC), triglycerides (TG), and fasting glucose levels were assessed using a Hitachi 7600 automatic chemistry analyzer (Hitachi, Tokyo, Japan). Direct LDLC measurements that were assessed by the automatic analyzer were used when available (participants eligible for sampling of heavy metal levels or with TG levels ≥200 mg/dL), and when unavailable, the Friedwald formula was used if the TG level was less than 400 mg/dL. Blood pressure was measured using a mercury sphygmomanometer (Baumanometer; WA Baum Co. Inc., Copiague, NY, USA) 3 times consecutively on the right arm with the participant in a seated position after at least 5 minutes of rest. The final blood pressure was obtained by averaging the second and third blood pressure measurements.12)
3. Definitions
Dyslipidemia was defined by levels of TC (≥240 mg/dL), HDLC (<40 mg/dL), TG (≥200 mg/dL), and LDLC (≥160 mg/dL, ≥130 mg/dL, or ≥100 mg/dL according to risk category) based on the National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III) guidelines,13) and whether participants answered that they were receiving treatment for dyslipidemia or taking medication to lower cholesterol levels.
Dyslipidemia awareness was assessed by the questions, “Have you been diagnosed with dyslipidemia by a doctor?" and “Are you currently suffering from dyslipidemia?" Patients who answered “yes" to either question were considered to be aware of their condition and assigned to the awareness group. Those who were diagnosed with dyslipidemia according to assessment of their lipid levels according to the NCEP-ATP III guidelines, but answered “no" to the aforementioned questions were included in the control group (unawareness group). Controlled dyslipidemia was also defined according to target levels set by NCEP-ATP III guidelines according to risk category.
Diabetes mellitus was identified based on fasting blood glucose levels (≥126 mg/dL) or use of insulin or oral hypoglycemic agents.14) Hypertension was diagnosed if subjects were taking medication for hypertension, or if average systolic blood pressure was over 140 mm Hg, or average diastolic blood pressure was over 90 mm Hg.15)
The study population was divided into two groups according to the definition of obesity (BMI ≥25 kg/m2) by the World Health Organization Regional Office for the Western Pacific Region and adopted by the Korean Society for the Study of Obesity.16)
4. Health Behavior for Control of Lipid Levels
Information related to health behavior that has been reported as being beneficial for the control of lipid levels was collected from the KNHANES V database, and these were divided into two groups: behavioral risk factors, and nutritional risk factors. KSLA 2015 and International Atherosclerosis Society (IAS) 2013 guidelines were used when applicable.
5. Behavioral Risk Factors
Information on current smoking status was collected through a self-reporting questionnaire, and those who answered that they smoked, or occasionally smoked, were considered current smokers, regardless of the amount. Smoking is a major cause of atherosclerotic cardiovascular disease (ASCVD), and the IAS states that high priority must be given to the prevention or cessation of smoking in lifestyle intervention for dyslipidemia.17)
Data on excessive alcohol consumption (≥3 standard drinks per occasion) were also collected through the self-reporting questionnaire. KSLA 2015 guidelines recommend limiting alcohol intake to 1–2 drinks per occasion.18)
Adequate physical activity was also assessed through answers to questionnaires and participants were considered to engage in adequate physical activity if they reported having carried out over 30 minutes of moderate intensity physical activity at least 5 days per week, or over 20 minutes of heavy intensity at least 3 per week. Epidemiological studies have shown that physical inactivity is associated with increased risk for ASCVD and regular physical activity has beneficial effects on lipoproteins.19) The IAS recommends approximately 30 minutes of daily moderate intensity activity, and specifies that the activity should be aerobic and carried out for a minimum of 5 days per week.17) For vigorous intensity activity, at least 20 minutes for 3 days a week was considered as adequate according to previous American Heart Association (AHA) guidelines.20)
6. Nutritional Factors
Nutritional factors were measured based on adherence to dietary recommendations that could be assessed using nutritional information provided by the KNHANES V. Therefore, adequate intake of macronutrients that was monitored by performing a 24-hour food recall and analyzed by the CAN-Pro software ver. 3.0 (Korean Nutrition Society, Seoul, Korea) was compared between the awareness groups. Adequate fiber intake (≥25 g/d), carbohydrate intake (<65% of total calories per day), fat intake (<30% of total calories per day), and protein intake (≥15% of total calories per day) were analyzed. The 2015 KSLA guidelines recommend limiting total daily carbohydrate intake and total fat intake to less than 30% of total calories per day and eating food rich in fiber for an intake of over 25 g of fiber per day.18) Diets high in cholesterol and saturated and trans-fat resulted in increased TG, LDLC, and total blood cholesterol. Previous studies have demonstrated that diets high in carbohydrate can increase TG levels, and dietary fiber can help lower blood cholesterol levels. For evaluation of protein and carbohydrate intake which was not specified in the 2015 KSLA guidelines, the American College of Sports Medicine recommendations were used where protein intake of 15% and carbohydrate intake of up to 60%–65% of total calories per day was prescribed for lifestyle management of dyslipidemia.21)
7. Statistical Analysis
All statistical analyses were performed using STATA statistical software ver. 14.0 (Stata Corp., College Station, TX, USA). All analyses were weighted to the Korean standard population from the years 2010 to 2012, reflecting the sampling method, response rate, and population structure of the KNHANES study.
Unpaired t-tests and chi-square tests were applied to continuous variables and categorical variables respectively in order to compare mean values and percentages of demographic and clinical characteristics between dyslipidemia patients according to awareness. Logistic regression was used to analyze which variables of health behavior were associated with awareness of dyslipidemia after adjusting for age. Afterwards, multivariable logistic regression was performed for each health behavior adjusting for age, education level, residential area (rural or urban), household income, self-perceived health status, marital status, and obesity (BMI ≥25 kg/m2). Adjusted OR, 95% confidence intervals (CI), and P-values were measured for the display of strength of each association. A P-value of <0.05 was considered significant.
Results
1. Baseline Characteristics of the Study Population
The characteristics of the study population are described in Table 1. Among the 6,624 dyslipidemia patients (14,415,037 when weighted), 17.1% were aware of their dyslipidemia status. Among the male population, 13.2% were aware of their diagnosis of dyslipidemia, while 22.6% of female dyslipidemia patients were aware of their diagnosis.
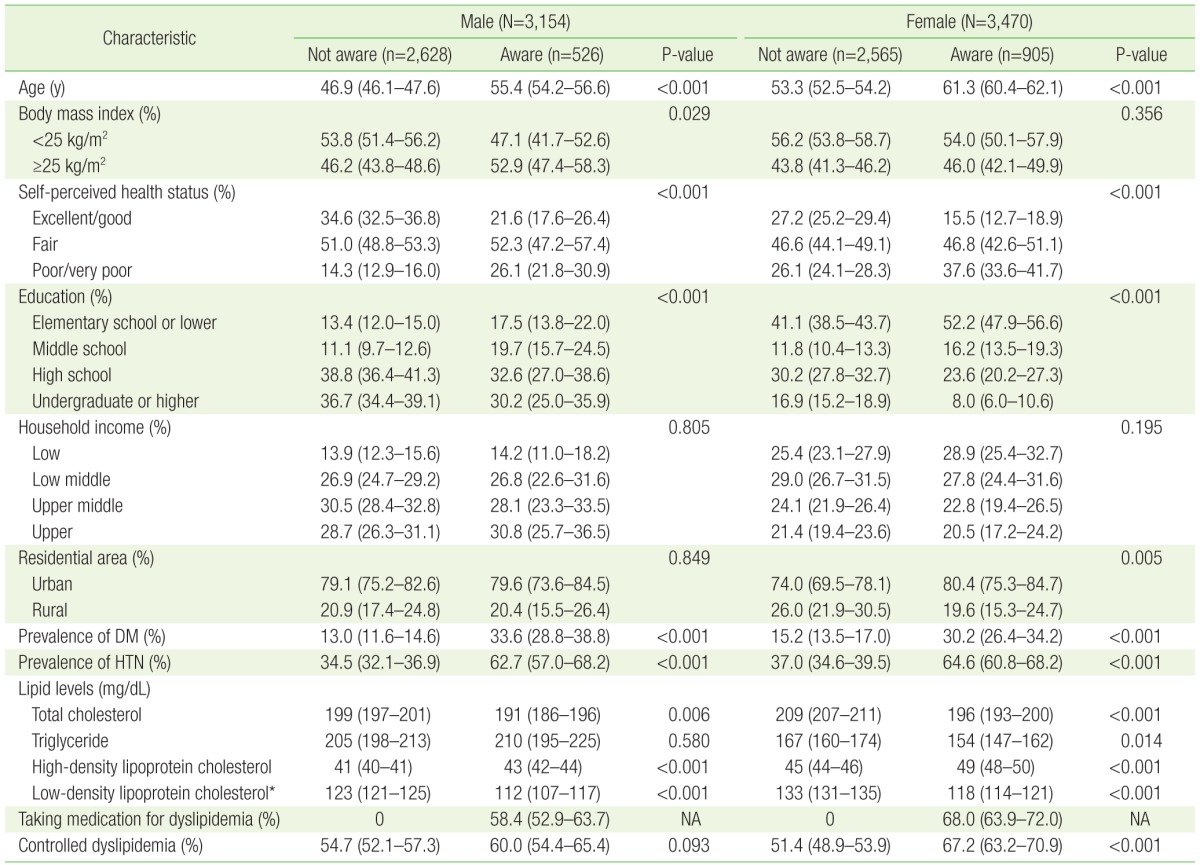
Characteristics of dyslipidemia patients according to awareness of dyslipidemia
The mean age of the group who were aware of their condition was higher than that of the group that was unaware in both men and women. With respect to self-perceived health status, 14.3% of male patients in the unaware group responded that their health status was poor or very poor while 26.2% of those in the aware group gave the same response. Among men, 13.4% of the unaware and 17.5% of the aware received an elementary school or lower level of education, while 41.1% of women unaware of their dyslipidemia status received an elementary school or lower level of education and 52.2% of aware women reported receiving the same degree of education.
Awareness of dyslipidemia in both male and female patients was associated with a higher prevalence of diabetes mellitus and hypertension. Lipid profiles were also significantly favorable in aware groups with higher HDLC levels and lower TC, TG, and LDLC levels in both male and female dyslipidemia patients, although differences in the level of TG was not statistically significant in men.
2. Health Behavior for Control of Lipid Levels
Both men and women who were aware of their diagnosis of dyslipidemia had lower current smoking percentages (38.5% and 3.6%, respectively), and fewer aware women were likely to consume alcohol in excess (23.8% vs. 13.5%). When adjusted for other characteristics, female patients in the awareness group had a lower current smoking rate compared with those in the unaware group (OR, 0.55; 95% CI, 0.32 to 0.94), but when adjusted for the prevalence of diabetes and hypertension, the result was not statistically significant (OR, 0.61; 95% CI, 0.35 to 1.06). As can be observed in Table 2, there were no significant differences for alcohol consumption or adequate physical activity.
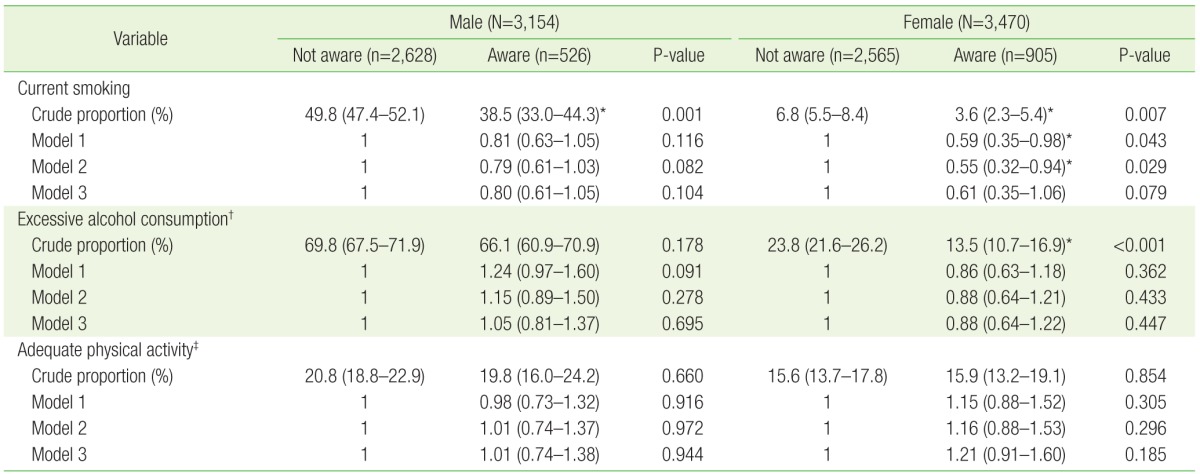
Behavioral risk factors according to awareness of dyslipidemia
3. Adequate Macronutrient Intake
The only favorable nutritional factor observed in the aware groups by crude proportions was adequate intake of fat found in women aware of their diagnosis of dyslipidemia (93.7% vs. 96.0%). Although female patients aware of their diagnosis showed a higher OR for adequate protein intake (OR, 1.26; 95% CI, 1.00 to 1.58) when adjusted for covariates, the result was not statistically significant when additionally adjusted for the prevalence of diabetes and hypertension (OR, 1.22; 95% CI, 0.98 to 1.53). Men also showed a higher OR for adequate intake of carbohydrate (OR, 1.33; 95% CI, 1.04 to 1.72), but when adjusted for diabetes and hypertension the result was not significant (OR, 1.28; 95% CI, 0.99 to 1.67). There were no other statistically significant differences as shown in Table 3.
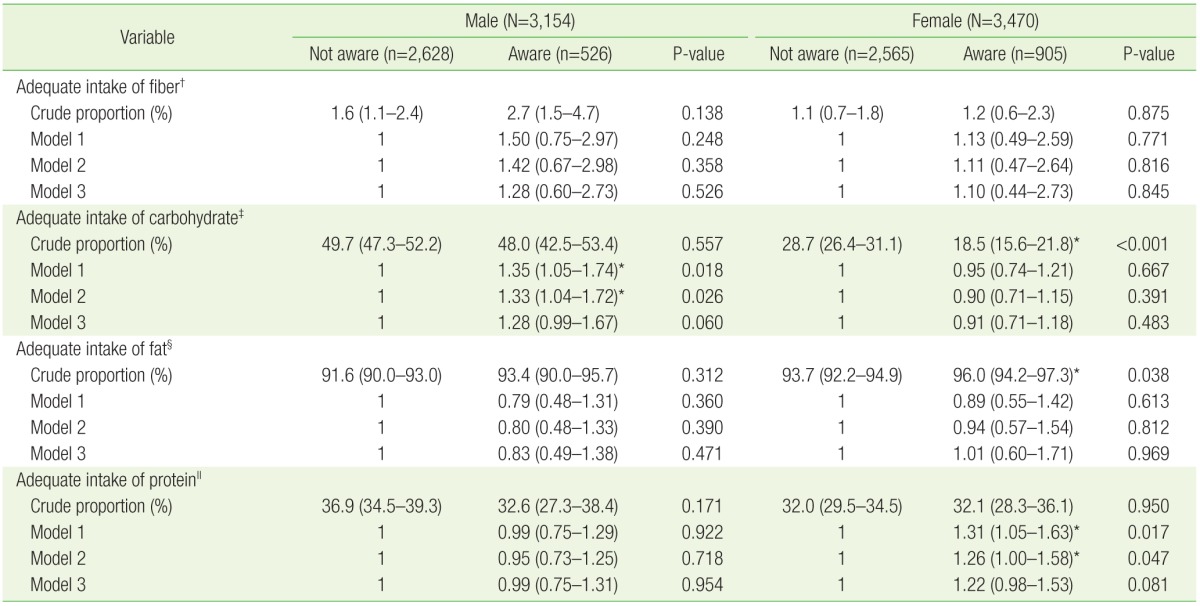
Nutritional factors according to awareness of dyslipidemia
4. Subgroup Analysis according to Prevalence of Diabetes and Hypertension
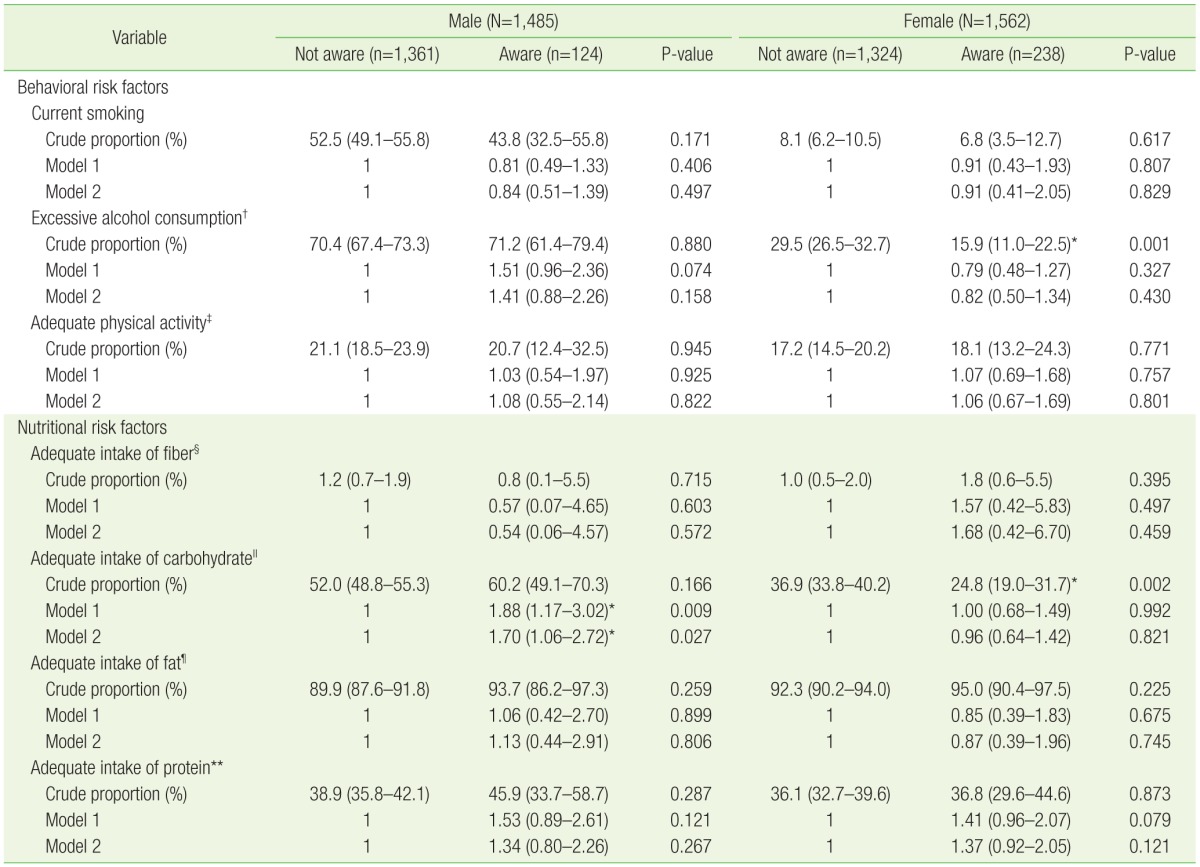
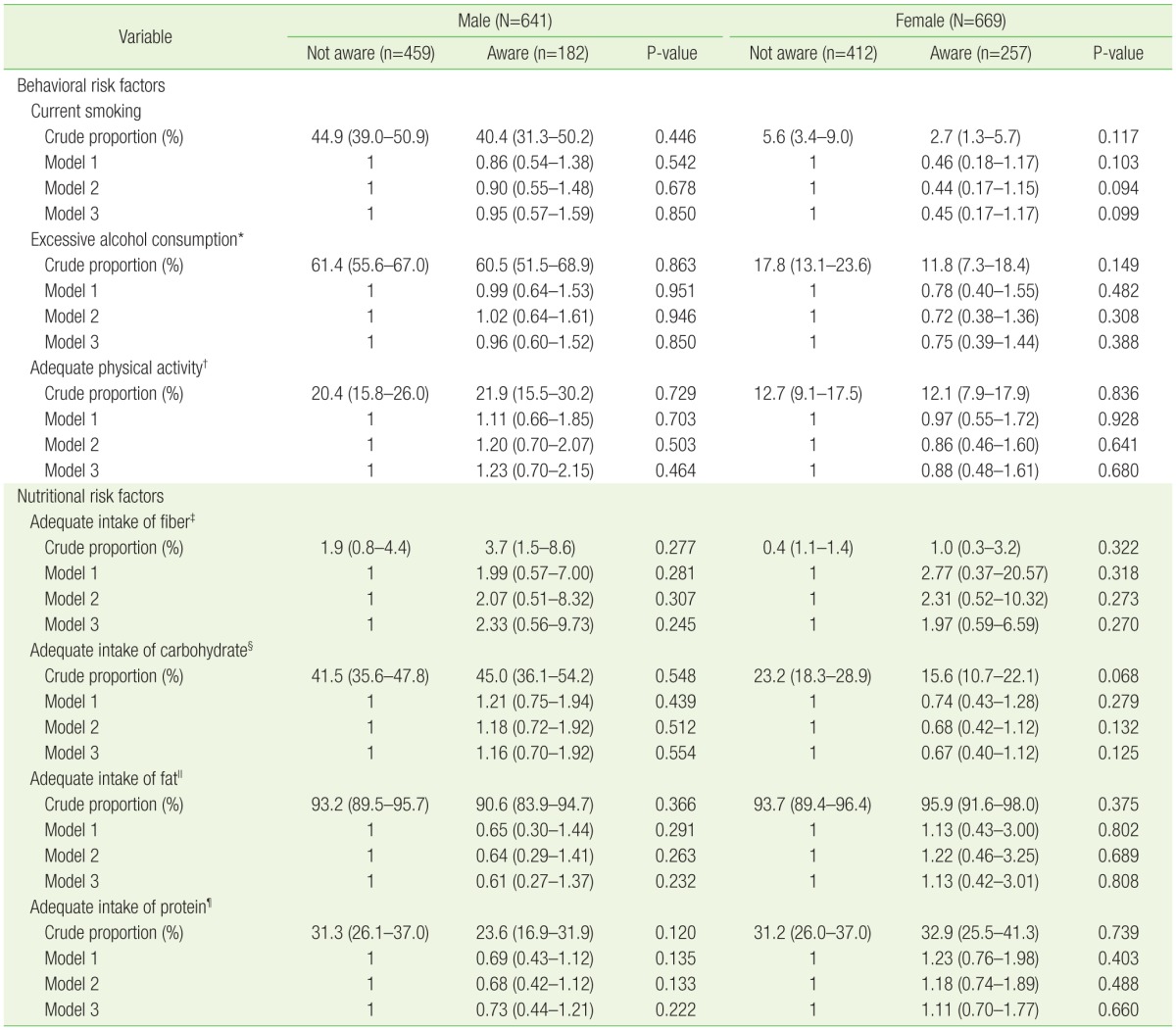
In subgroup analysis of dyslipidemia patients without either hypertension or diabetes, men aware of their diagnosis of dyslipidemia had a higher OR for adequate carbohydrate intake (OR, 1.70; 95% CI, 1.06 to 2.72) after adjusting for other factors (Table 4).
Subgroup analysis of health behavior according to awareness of dyslipidemia in subjects without hypertension or diabetes mellitus
In the subgroup analysis of dyslipidemia subjects with diabetes mellitus, there were no significant differences in health behavior according to awareness (Table 5). In the subgroup analysis of dyslipidemia subjects with hypertension, aware women showed a lower OR for smoking (OR, 0.46; 95% CI, 0.24 to 0.91) and a higher OR for adequate protein intake (OR, 1.37; 95% CI, 1.03 to 1.84), but when adjusted for covariates the results were no longer statistically significant (Table 6).
Subgroup analysis of health behavior according to awareness of dyslipidemia in subjects with diabetes mellitus
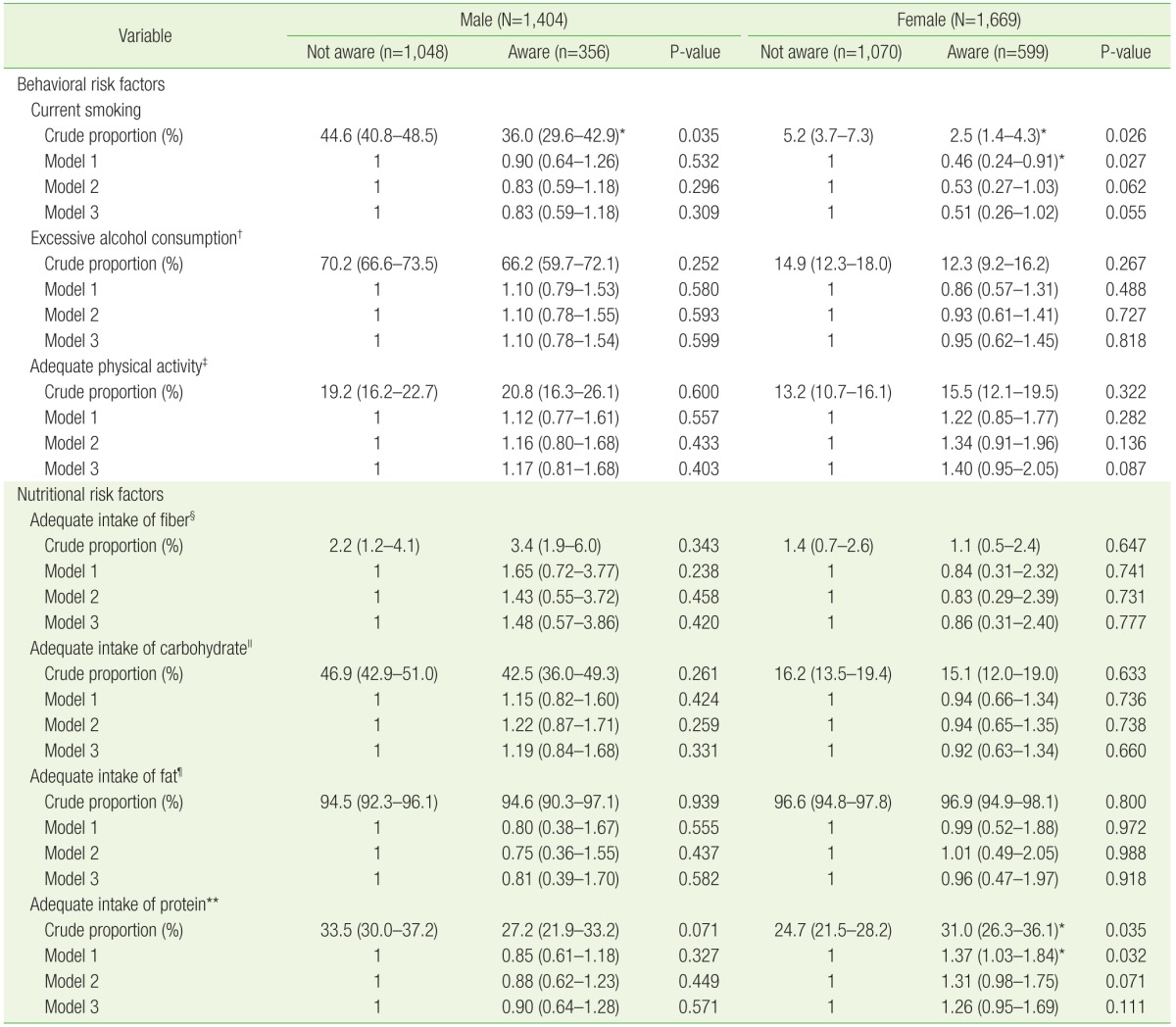
Subgroup analysis of health behavior according to awareness of dyslipidemia in subjects with hypertension
Discussion
This study suggests that there is minimal difference in health behavior between those aware and those unaware of their diagnosis of dyslipidemia among Korean adults over the age of 20 years. There was no statistically significant difference in health behavior and adequate macronutrient intake between the awareness groups after adjusting for demographic variables and the prevalence of diabetes and hypertension, perhaps because diabetes and hypertension are more important factors influencing adherence to health behavior. The only beneficial health behavior was found in the subgroup analysis, where adequate carbohydrate intake was observed in men with neither hypertension nor diabetes.
When analyzing crude proportions of adequate health behavior, rates of current smoking (38.5%) and excessive alcohol consumption (66.1%) in men aware of their diagnosis of dyslipidemia were higher than desirable and rates of adequate physical activity in both male and female dyslipidemia patients (19.8% in aware men and 15.9% in aware women) showed rates with ample room for improvement. Although rates of adequate fat intake were high in patients with dyslipidemia (93.4% in aware men and 96.0% in aware women), adequate intake of fiber in all subjects (2.7% in aware men and 1.2% in aware women), and carbohydrate in women (18.5% in aware women) were comparatively low. These results show that there is room for improvement in health behavior in the general population with dyslipidemia, even in those aware of their conditions. Unfortunately, awareness was not significantly associated with the health behaviors mentioned above after adjustment for covariates, implying that merely increasing awareness is not enough to promote health behavior. However, causality cannot be determined due to the cross-sectional design of this study.
Adequate control of lipid levels is important. A 1% reduction in total serum cholesterol levels can lead to a 2% to 3% reduction in risk of coronary disease,22) and a meta-analysis revealed that a 10% reduction in serum cholesterol was linked to a 13% to 14% reduction in CHD mortality and 8% to 10% reduction in total mortality.23) Although treatment of dyslipidemia with medication is important for adequate control of lipid levels, associated health behaviors and education for their implementation are also of importance and several guidelines (KSLA 2015, NCEP-ATP III, and IAS 2013 guidelines) actively recommend lifestyle intervention after diagnosis. In the study performed on dyslipidemia patients under pravastatin treatment in Japan, high awareness of health and positive attitude towards diet and exercise, and high adherence to drug therapy were related with favorable overall lipid levels.9)
Results published by the Korean Ministry of Health and Welfare on data from the KNHANES reveal that awareness rates of dyslipidemia are steadily rising (24.0% in 2005 to 59.0% in 2013); however, it is still low when compared to published results of awareness of other chronic diseases such as hypertension (65.3% in 2013) and diabetes (74.3% in 2013).24) The diagnosis and improved awareness of dyslipidemia are critical first steps for its adequate management; results in this study show that lipid profiles were more favorable for both men and women aware of their condition which may have been the result of lipid-lowering agents. Use of medication is inevitably higher in groups aware of their condition, as can be observed in the baseline characteristics of subjects for this study. Because there were no significant differences in adherence to health behavior recommended by clinical guidelines except for adequate carbohydrate intake in men with neither hypertension nor diabetes and rates of several types of health behavior showed plenty of room for improvement, adherence to health behaviors must be emphasized. Such change in behavior can be expected to have additional beneficial effects on lipid levels.
Although additional long-term studies are required to evaluate whether awareness of dyslipidemia can affect health behavior, results of this study suggest that awareness of dyslipidemia alone may not be enough to promote health behavior. One explanation can be that patients may be lacking in proper dyslipidemia education and instruction from their healthcare providers. This may also be the case for other chronic diseases. A study carried out on KNHANES 1998–2012 data analyzing adherence to dietary recommendations among Korean adults with diabetes mellitus concluded that Korean patients with diabetes have poor adherence to dietary recommendations and healthy lifestyle published by the Korean Diabetes Association regardless of awareness of diabetes.25) However, another study by Bardenheier et al.26) showed that both men and women aware of their diagnosis of diabetes differed in their daily intake of sugar and protein when compared to those unaware of their diabetic status. Although the difference in outcome may be due to the varied definitions of factors analyzed for association with awareness, the disparities between these studies may suggest that other factors exist apart from awareness influencing adherence to health behavior, and that the role of healthcare providers and practitioners may be crucial for lifestyle modification. Although well-established guidelines for chronic diseases call for lifestyle change as the initial line of therapy, it has been reported that physicians often do not follow these practices.27) Correct insights for medical professionals with respect to guidelines in the management of dyslipidemia, and monitoring and support systems may be required for better lifestyle behavior. Further studies are needed to provide insight on attitudes of both physicians and patients towards management of dyslipidemia through lifestyle interventions.
The development and establishment of public health policies to promote adequate behavior for the management of dyslipidemia may also be of help. A project carried out in Finland found that health promotion campaigns at a national level through various activities (such as media campaigns and health fares) can help increase population awareness on prevention of chronic diseases and prompt subjects to make beneficial lifestyle changes.28) Issues such as the perception of severity of risk factors and diseases, benefits of lifestyle modification, and calls to action should be addressed.29) As a further step, a multi-team approach and cooperation between healthcare providers and the community can provide fully integrated care leading to improved awareness and management of dyslipidemia.
In addition, interventions at community levels may also be helpful. Fritsch et al.30) reported that lipid-based interventions at the worksite (education and coaching on lifestyle and lipid values through classes and phone call interventions) can improve lifestyle behavior including exercise and diet, contribute to continuous health care, and lead to improved lipid values. After a 7-month intervention program, participants had an average of 5.2% reduction in TC.30) However, this was a short-term study performed at companies that were all members of a health insurer in North Carolina. Further large-scale studies carried out for a longer time intervals, or randomized controlled trials may be required to identify intervention methods that can effectively enhance health behavior in dyslipidemia patients.
This study has several strengths. First, to the knowledge of the authors, this is the first study to analyze adherence to health behavior recommended by clinical guidelines for the management of dyslipidemia according to patients' awareness. Furthermore, this study was conducted using data from a nationally representative sample of the Korean population, making the estimates of this study generalizable to the population of dyslipidemia patients in Korea. Additionally, KNHANES provides data collected through standardized laboratory and physical measurements. Finally, data was used from three consecutive years, providing a large sample size and powering the statistical ability to report associations.
This study also has several limitations. Because it is based on a cross-sectional design, it is difficult to assess any temporal relationship between awareness of dyslipidemia and health behavior and adequate macronutrient intake. Although daily intake of macronutrients was assessed for nutritional factors due to limited information and lack of data on total daily cholesterol intake or level of saturated or trans-fatty acids, evaluation of dietary patterns (such as AHA 2020 ideal healthy diet or Mediterranean diet) may be more appropriate due to inconclusive evidence of an independent effect of macronutrient intake on outcomes.31) Furthermore, it is unclear whether the status of each health behavior that the subjects reported would continue long term. There is also a need for the consideration of recall and social desirability bias, since data collected through self-reporting questionnaires was used for this study.
In summary, this is the first national-level study to analyze adherence to health behavior stipulated by clinical guidelines (by the KSLA and IAS) in dyslipidemia patients according to awareness. In this study, awareness was not associated with adequate health behavior except for adequate carbohydrate intake in men found in subgroup analysis of dyslipidemia subjects without hypertension or diabetes. Although further studies are required to assess any temporal relationship between awareness and health behavior, development of procedures including counseling and education by healthcare providers could be considered to guide patients according to guidelines for optimal control of lipid levels and prevention of CVD. Furthermore, large-scale prospective cohort studies that can help define reliable and practical plans for the enhancement of healthy behavior for the management of dyslipidemia are needed.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.