INTRODUCTION
With improvements in cancer screening and treatment, there are cur-rently over 13 million cancer survivors in the Unites States.1) In Korea, the estimated number of cancer survivors was more than 1 million,2) and the 5-year relative survival rate was almost 68% in 2012.3)
Cancer survivors have more co-morbidities and an elevated risk of non-cancer mortality compared to the general population.4,5) Cardiovascular disease (CVD) is the most frequent cause of morbidity and mortality in cancer survivors, following second primary cancer.6,7) and the most common cause of non-cancer mortality in cancer survivors, accounting for 31% of these deaths in Korea.8)
There are several factors that increase the risk of CVD among cancer survivors. First, cancer survivors are usually older than the general population. Second, cancer survivors have risk factors that are common for both cancer and CVD (e.g., obesity, smoking, and physical inactivity).7,9) Third, the late cardiotoxic effects of cancer therapies (e.g., radiation and chemotherapy) have been associated with increased CVD risk.6,7,10,11) Fourth, lifestyle changes after cancer treatment (e.g., weight gain and reduced physical activity) may well exacerbate the risk of CVD.
Therefore, continuous monitoring and aggressive management of modifiable cardiovascular risk factors may reduce some of the CVD burden in cancer survivors.12) Prior studies have noted suboptimal control of CVD risk factors, such as physical inactivity, smoking habits, and obesity, in cancer survivors.13,14) Additionally, recent studies have shown that CVD risk factors are more common among cancer survivors than among the general adult population.6,7)
However, no studies have examined a large set of CVD risk factors or the anticipated overall CVD burden in adult cancer survivors. In this study, to emphasize the importance of prevention and management of CVD in cancer survivors, we assessed modifiable traditional CVD risk factors and the risk of future CVD events among cancer survivors in comparison to the general population. The risk of future CVD events was estimated as the 10-year probability of CVD using the Framingham risk score, derived from the Framingham Heart Study, the most commonly used CVD risk score worldwide.15,16) We hypothe-sized that cancer survivors would have a higher CVD risk and 10-year probability of CVD than the control groups.
METHODS
1. Data Source
The current study was based on data obtained from the 2007–2013 Korea National Health and Nutrition Examination Survey (KNHANES IV–VI). The KNHANESs are cross sectional nationwide surveys that represent the general Korean population, and are performed by the Korea Centers for Disease Control and Prevention.
These surveys use a stratified, multistage probability sampling design according to geographic area, sex, and age group to select a representative sample of the civilian, non-institutionalized Korean population. The KNHANES survey is composed of a health interview, health examination, and nutrition survey. We used data from the health interview and health examination survey that asked questions pertaining to socio-demographic characteristics, health status, medical history, and physiological status. This study was conducted under the approval of the institutional review board of the Samsung Medical Center (IRB no. SMC 2015-02-031). Informed consent was waived by the ethics committee because this study was based on a retrospective analysis of existing administrative and clinical data.
2. Study Population
We combined data from the 2007–2013 surveys into a large cross-sectional dataset. A total of 58,423 subjects participated in the KNHANES IV–VI. To limit the analysis to adults, we excluded individuals under the age of 20 years. Participants with missing data were also excluded. Our final study sample consisted of 1,225 cancer survivors and 5,196 subjects with no history of cancer (non-cancer controls) (Figure 1). Patients were considered to be cancer survivors from the time of diagnosis through the remaining years of life, using the definition of the National Coalition for Cancer Survivorship.
3. Definition of Variables
Sociodemographic characteristics included age, sex, education level (high school diploma, beyond high school), marital status (single, married), and household monthly income (<3,000 US dollar [USD], ≥3,000 USD). Co-morbidities were defined based on self-reported histories of hypertension, stroke, myocardial infarction or angina, and dyslipidemia or diabetes mellitus. Participants consuming alcohol were classified as risky drinkers, nondrinkers, or non-risky drinkers. Risky drinking was defined as alcohol consumption exceeding 3 standard drinks per day. We classified the participants as cancer survivors if they answered "yes" to the following question: "Have you ever been told by a doctor that you have any kind of cancer?" The type of cancer and the age at diagnosis were also noted. The time since cancer diagnosis was calculated by subtracting the participant's age at the time of diagnosis of cancer from their present age.
CVD risk was assessed based on modifiable cardiovascular risk factors and the 10-year probability of CVD. According to the American Heart Association (AHA)/American College of Cardiology guidelines, tobacco use, physical inactivity, high blood pressure, high cholesterol level, obesity, and elevated blood glucose level are the traditional modifiable cardiovascular risk factors.17) In this study, a total of 10 cardiovascular risk factors were assessed, and each variable was classified into two groups as follows: Blood pressure was assessed for systolic and diastolic pressures (140 mm Hg and 90 mm Hg, respectively). Smoking status was defined as current, non-, or ex-smoker. Blood chemistry findings were as follows: total cholesterol <200 mg/dL; high density lipoprotein cholesterol (HDLC) <40 mg/dL in males and <50 mg/dL in females; low density lipoprotein cholesterol (LDLC) <160 mg/dL; fasting glucose <126 mg/dL; hemoglobin A1c (HbA1c) <6.5%; and body mass index (BMI) <25 kg/m2. Based on physical activity, the subjects were classified into either the active group (moderate physical activity for at least 30 minutes per day, 5 days per week or vigorous physical activity for at least 20 minutes per day, 3 days per week) or the inactive group (no physical activity or insufficient physical activity).
4. Estimation of 10-Year Probability of Cardiovascular Disease
The 10-year probability of CVD was estimated using the Framingham risk score. These scores included the cancer survivors and non-cancer controls aged between 30 and 74 years and without CVD at the baseline examination by the Framingham heart study.15)
The variables used to calculate the Framingham risk score are age, systolic blood pressure, use of antihypertensive therapy, presence of diabetes mellitus, smoking habits, total cholesterol level, and HDLC level. CVD outcomes included coronary death, myocardial infarction, coronary insufficiency, angina, ischemic stroke, hemorrhagic stroke, transient ischemic attack, peripheral artery disease, and heart failure.15)
5. Statistical Analysis
All statistical analyses were performed using the IBM SPSS Statistics software ver. 22.0 (IBM Co., Armonk, NY, USA). Continuous variables were expressed as the mean±standard error. Categorical variables were compared using a chi-square analysis. Univariate logistic analysis was conducted to evaluate related CVD risk factors for the cancer survivors and non-cancer controls. In addition, we estimated the mean value of the 10-year probability of CVD in the subjects using a complex samples general linear model. Statistical significance was defined as a P-value of ≤0.05.
RESULTS
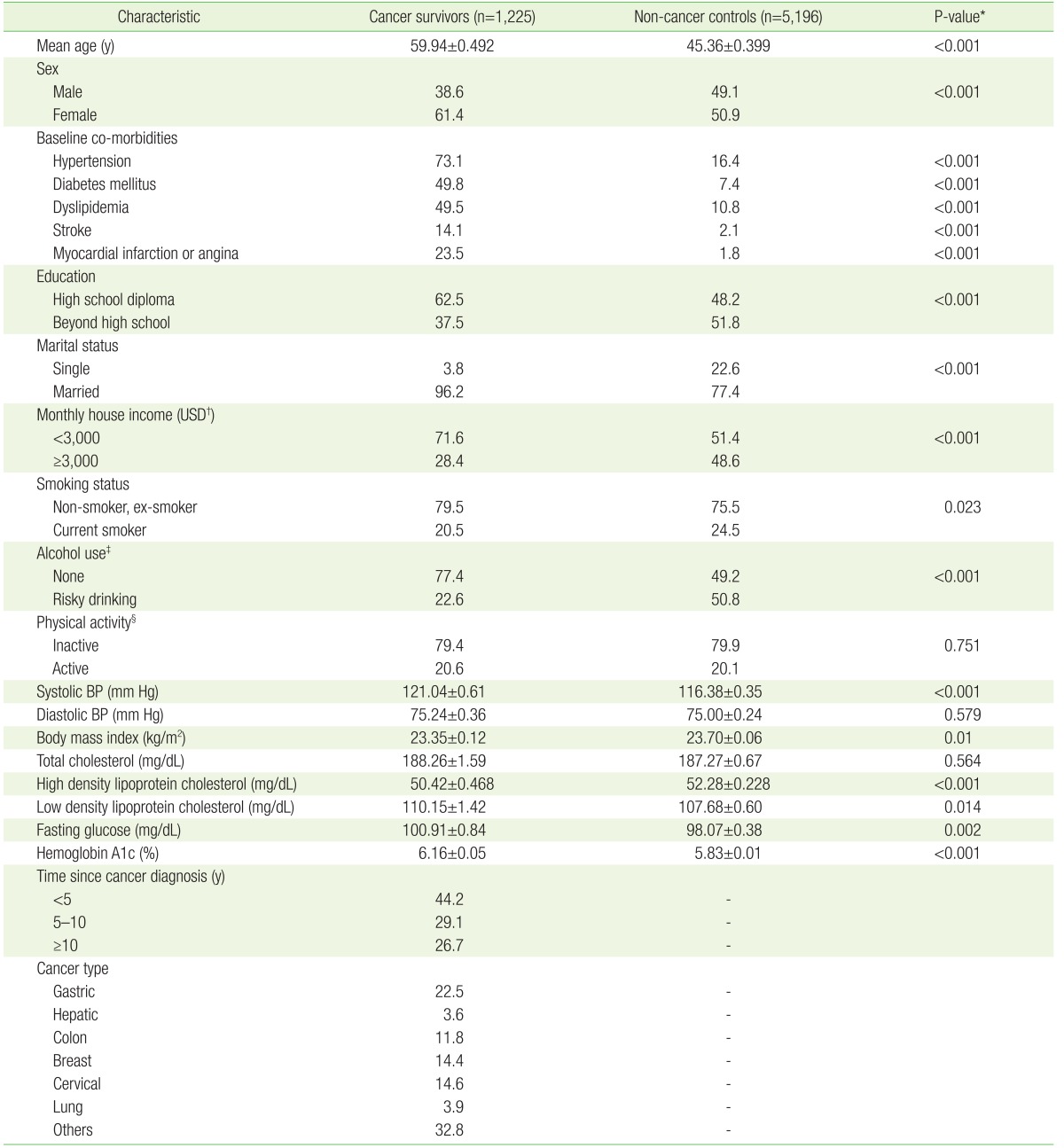
Baseline characteristics of the study population by cancer status are presented in Table 1. After excluding the participants with missing values, a total of 1,225 cancer survivors and 5,196 non-cancer controls were identified (mean age, 59.9 and 45.3 years, respectively). The cancer survivors were more likely to be older, female, married, and have a lower level of education and monthly income. In the cancer survivor group, the percentage of risky drinkers and current smokers, and mean BMI were significantly lower than in the control group, while mean systolic blood pressure and HDLC, LDLC, fasting glucose, and HbA1c levels were significantly higher in the cancer survivors than in the controls. The most common co-morbidity was hypertension. Approximately 37.6% of the cancer survivors had a history of CVD, which included stroke, myocardial infarction, or angina.
Of the 1225 cancer survivors, 63.3% reported having one of the following four types of cancer: stomach (22.5%), cervical (14.6%), breast, (14.4%), or colon (11.8%), and 44.2% of the cancer survivors were diagnosed as having had the disease for less than 5 years.
1. The Cardiovascular Disease Risks in Cancer Survivors versus the Control Group
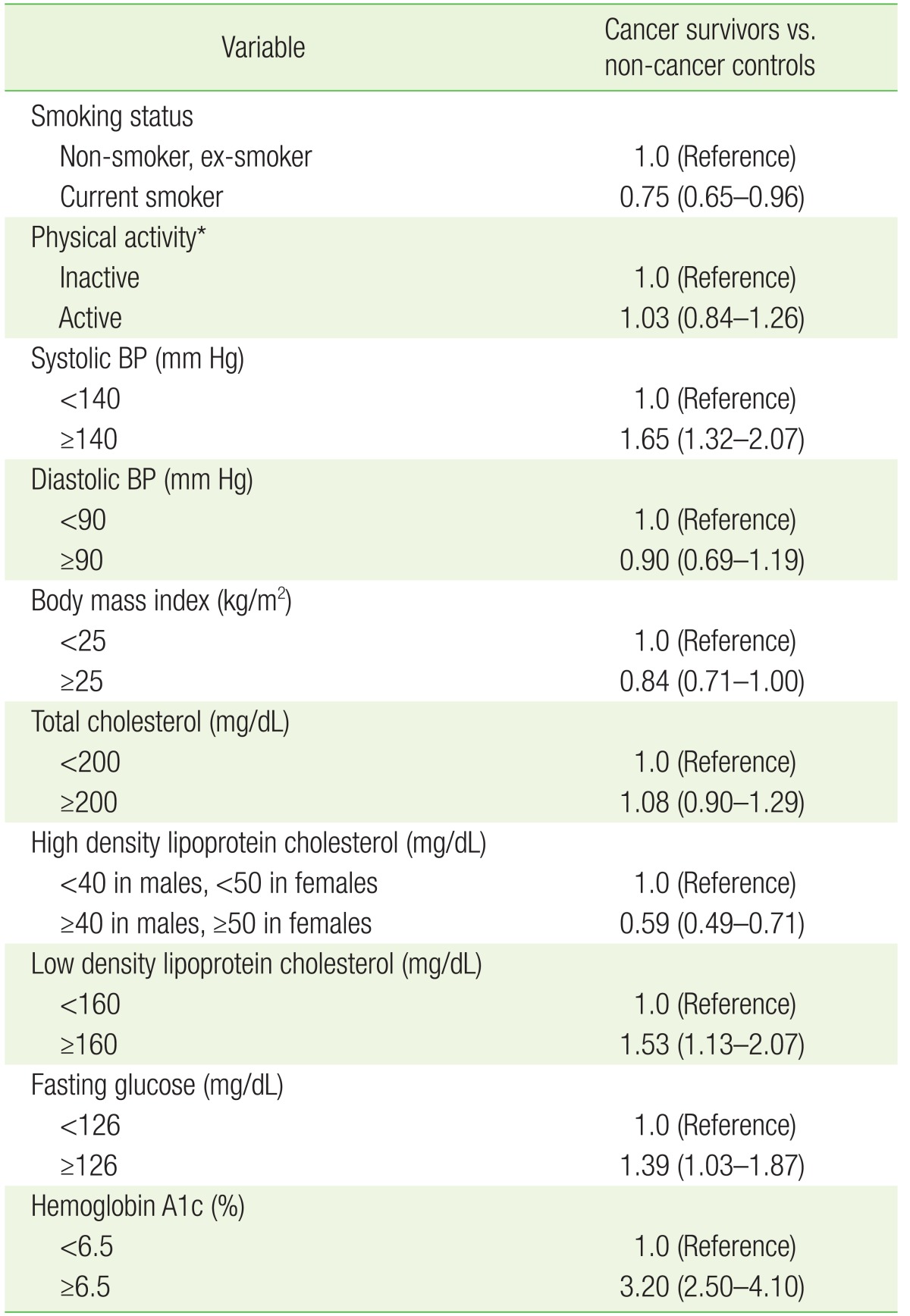
To evaluate the CVD risk in the cancer survivors, a univariate logistic analysis was performed. Smoking status, systolic blood pressure, and fasting glucose, HbA1c, LDLC, and HDLC levels were significantly and independently associated with cancer history (P<0.05). The cancer survivors were more likely to be classified as never- or ex-smokers than the non-cancer controls (odds ratio, 0.75; 95% confidence interval, 0.13 to 0.89). The proportion of subjects who had higher fasting glucose levels, HbA1c levels, systolic blood pressure, and LDLC levels, and lower HDLC levels was significantly higher in the cancer survivors than in the non-cancer controls (Table 2).
2. Ten-Year Probability of Cardiovascular Disease Base on the Framingham Risk Score
The average 10-year probability of CVD was 19.1% for the cancer survivors and 13.3% for the non-cancer controls (Figure 2A). In both men and women, the average 10-year probability of CVD among the cancer survivors was higher than among the non-cancer controls (men: 27.0% for cancer survivors and 20.8% for non-cancer controls, women: 12.5% for cancer survivors and 6.7% for non-cancer controls) (Figure 2B).
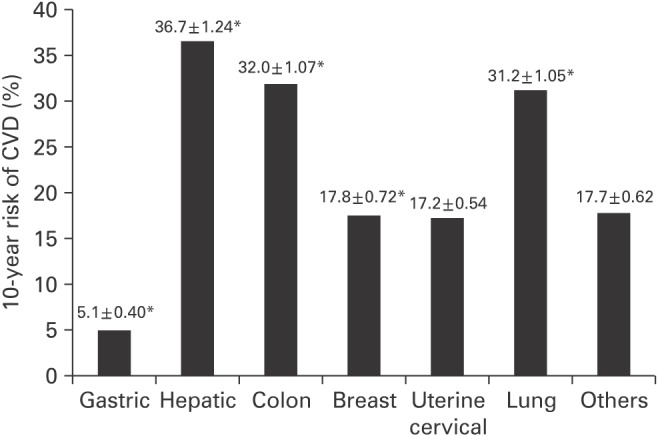
The average 10-year probability of CVD according to the cancer type was significantly higher for the patients with hepatic, colon, lung, breast, and gastric cancer than for the non-cancer controls (36.7% for hepatic cancer, 32% for colon cancer, 31.2% for lung cancer, 17.8% for breast cancer, 17.7% for cervical cancer, 5.1% for gastric cancer) (Figure 3).
DISCUSSION
The major finding of the present study is that the proportion of subjects who had higher fasting glucose and HbA1c levels, systolic blood pressure, and LDLC levels, and who had lower HDLC levels was significantly higher in Korean cancer survivors than in the non-cancer controls. The 10-year probability of CVD was also higher among the cancer survivors in both men and women, and significant variation existed in relation to the cancer type.
The behaviors related to the risk of CVD among cancer survivors, such as smoking, physical inactivity, and obesity, have been investigated in several surveys. Smoking is a well-known cause of cancer. A sig nificant number of studies have reported similar rate of smoking in cancer survivors compared with the general population.9,13,18,19) In contrast, our study showed that current smoking rates were significantly lower in cancer survivors, which is consistent with prior studies report-ing a lower rate of current smoking among cancer survivors.7,20) These contradictory results might be explained by two possibilities. First, there is the possibility that the smoking rate might be underestimated due to the selective survival and a small number of smoking-related cancers. Second, cancer survivors were more likely to be ex-smokers who had undergone smoking cessation education.
Only 20.6% of the cancer survivors met the AHA recommended level of physical activity, and there was no significant difference in the activity level compared to the non-cancer controls. Similar findings were observed in a recent study in the US.9) However, these results differ from those of a previous study reporting that 58% of prostate and breast cancer survivors engaged in routine exercise after treatment.21) The reasons for these differences may be as follows. First, physical activity goals were set differently because there are no definite exercise guidelines for cancer survivors.14) Second, there are likely to be differences in physical activity in relation to survival time and the type and stage of cancer in cancer survivors.
Weaver et al. found that being overweight and obese was more common in breast, prostate, colorectal, and gynecologic cancer survivors,7) and several previous studies have reported higher BMI in breast and prostate cancer survivors22,23,24) and lower BMI in esophageal and gastric cancer survivors.25,26) In our study, BMI was lower in the cancer survivors than in the non-cancer controls but the difference was not significant. There is a possibility that a lower BMI in the cancer survivors may be a result of the cancer itself. Additionally, various confounding factors also may distort the relation between BMI and cancer history sta-tus.
In addition, our study examined control of the objective CVD risk factors, such as blood pressure, lipid profile, and fasting glucose level among cancer survivors compared with the general population. Except for diastolic blood pressure and total cholesterol level, the other measured CVD risk factors were higher in the cancer survivors. In recent surveys in the US, no significant differences were found in the proportion of cancer survivors with hypertension or hypercholesterolemia.9) Meanwhile, long-term survivors of metastatic testicular cancer had higher blood pressure and had hypercholesterolemia.27) In another study, hypertension and diabetes were common in breast, prostate, colorectal, and gynecologic cancer survivors.7) However, to our knowledge, no study has examined the overall modifiable risk factors for CVD among cancer survivors.
To our knowledge, no study has examined the risk of future CVD events in adult cancer survivors. We predicted the average 10-year probability of CVD using the Framingham risk score.15) The average 10-year probability of CVD in cancer survivors was higher than in non-cancer controls, in both men and women. Additionally, there was a significant difference in the average 10-year probability of CVD in relation to the cancer type; it was significantly higher in hepatic, colon, lung, breast, and gastric cancer (listed in decreasing order of probability).
In our study, the average 10-year probability of CVD in men was 27% for cancer survivors and 20% for non-cancer controls, and in women, it was 12% for cancer survivors and 6% for non-cancer controls. Several recent studies have demonstrated that the Framingham risk score overestimates the CVD risk in Asia,28) including Korea.29,30) In a recent Korean nationally representative prospective cohort study, the average 10-year risk for coronary heart disease was 1.03% for men and 0.40% for women during an 11.6-year median follow-up, while the Framingham risk score predicted 3–6 times as many coronary heart disease events than observed.30) Moreover, the non-cancer control group in this study was heterogeneous, including unhealthy individuals with a number of co-morbidities. Therefore, the overall 10-year probability of CVD in our subjects is likely to have been overestimated from the actual incidence of CVD. However, we have to consider that our study also examined the 10-year probability of CVD including stroke, peripheral artery disease, and heart failure, as well as that of coronary heart disease.
This study has some limitations related to the use of the KNHANES data. First, the KNHANES was not designed to evaluate cancer survivorship. Thus, the number of cancer survivors in the study was relatively small that might have limited the significance of the results, the ability to generalize our results to all cancer survivors in Korea, and the conducting of further analysis. Second, we did not have information on CVD risk factors and health behaviors prior to the cancer diagnosis in the KNHAES data. Although CVD risk was higher in cancer survivors, it is difficult to establish a sequential relationship between cancer and CVD risk. Third, the KNHANES did not include information on cancer treatment status. Therefore, we were not able to determine the cancer stage or the proportion of cancer survivors who received active treatment and were eventually symptom free. In addition, we could not evaluate if cancer survivors received treatment methods linked with cardiotoxicity, which may have influenced our results. Therefore, future studies need to examine the control of CVD risk in cancer survivors with a well-documented treatment history. Finally, self-reported cancer, history of other chronic disease, and health behavior are all subject to recall or misclassification bias.
Despite these limitations, our findings suggested that cancer survivors had a higher CVD risk and10-year probability of CVD than the non-cancer controls. Our study also emphasizes that optimal control of CVD risk factors for preventing CVD and reducing non-cancer-related death is important in treating cancer survivors. These findings suggest that the rates of receiving adequate treatment for CVD risk factors were lower in cancer survivors than in the general population.
Therefore, CVD risk management and a well-defined CVD prevention program are needed for cancer survivors. For this, primary care physicians and cancer specialists should work together to oversee appropriate surveillance and modification of CVD risk factors. Cancer survivors and their caregivers also need to recognize the risk of CVD and manage the risk factors aggressively.