INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is characterized by chronic inflammation of the airways, lung parenchyma, and pulmonary vasculature, causing airflow limitation that is not fully reversible.1) COPD is a known cause of secondary polycythemia with elevated erythropoietic demands in response to the consequent hypoxemia. However, anemia is relatively common in patients with COPD and is related to increased mortality.2) Indeed, anemia-accompanied COPD has been shown to be independently related to incremental costs of $3,582 per patient per year according to data from United States Medicare claims.3)
A number of previous studies have shown decreased iron availability in COPD patients. Low-grade systemic inflammation in COPD may represent a possible cause of anemia in this chronic disease.4) More specifically, impaired iron availability results from upregulation of ferritin mRNA due to elevations in the levels of inflammatory cytokines such as interleukin-1 and interferon-c.5) In addition, certain inflammatory cytokines, such as tumor necrosis factor and interleukin-1, are thought to be related to reduced iron utilization,6) and one study suggested the presence of erythropoietin resistance in anemic COPD patients presenting with high erythropoietin levels, a phenomenon that is probably regulated through inflammatory mechanisms.7)
The iron status in patients with COPD reflects the balance between the stimulation of erythropoiesis by hypoxia and its depression by inflammation. The present study was conducted to determine whether the various iron parameters are associated with the severity of COPD. We measured the serum hemoglobin (Hb) and several iron parameters, including serum iron, ferritin, transferrin saturation (TSAT), and the total iron-binding capacity (TIBC), in patients with COPD, and their relation to the forced expiratory volume in 1 second (FEV1), as an indicator of COPD severity.
METHODS
1. Study Design
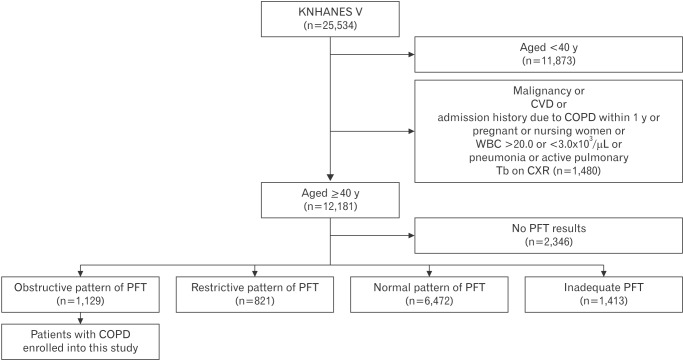
We performed a cross-sectional cohort study using data from the fifth Korean National Health and Nutrition Examination Survey (KNHANESV), a nationally representative stratified random sample of the Korean population in 2010ŌĆō2012. A flowchart for the study cohort selection procedure is presented in Figure 1. The survey involved subjects aged Ōēź40 years who had undergone complete spirometry measurements. The exclusion criteria included malignancy, cardiovascular disease, admission history due to COPD within the past year, pregnant or nursing women, white blood cell count of Ōēź20.0 or Ōēż3.0├Ś103┬Ą/mL, pneumonia or active pulmonary tuberculosis on chest radiograph, a restrictive or normal pattern identified by pulmonary function test (PFT), or an inadequate PFT. The clinical diagnosis of COPD was confirmed using the Global Initiative for Chronic Obstructive Lung Disease criteria.8) COPD was defined as an FEV1/forced vital capacity ratio <0.70.
2. Measures of Iron Status and Anemia
We examined the Hb level and iron status using laboratory measures for serum iron, ferritin, and TIBC. TSAT was calculated as follows: TSAT (%)=serum iron├ĘTIBC├Ś100.
3. Statistical Analyses
Data analyses were performed using IBM SPSS Statistics ver. 23.0.0.0 (IBM Corp., Armonk, NY, USA). The associations between FEV1 and the variables were evaluated using Spearman correlations. Multiple linear regression analysis was used to evaluate the relationships between FEV1 and the variables after adjusting for age, sex, and body mass index (BMI). Normally distributed continuous variables are expressed as the mean┬▒standard deviation. Non-normally distributed continuous variables are expressed as the median (minimumŌĆōmaximum) value. For all analyses, a P-value of less than 0.05 was considered statistically significant.
RESULTS
1. Characteristics of the Subjects
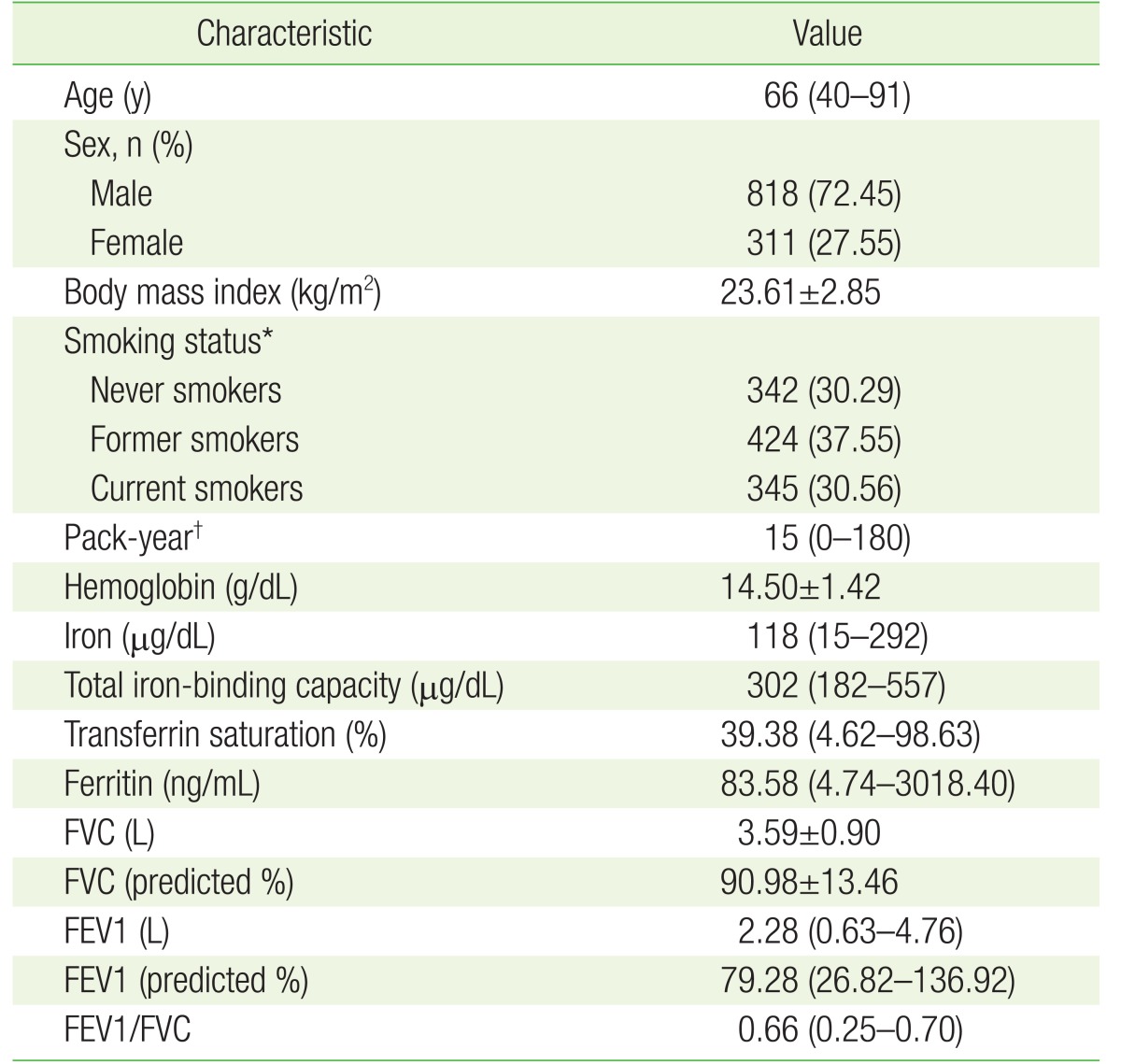
The baseline characteristics of the cohort are shown in Table 1. The median age of the cohort was 66 years (range, 40ŌĆō91 years). There were fewer female (27.55%) than male (72.45%) patients with COPD. The proportion of smokers (68.11%) was higher than that of never-smokers (30.29%). The median (minimumŌĆōmaximum) number of smoking pack-years was 15 (0ŌĆō180).
2. Associations of FEV1 with Hemoglobin and Iron Parameters in Chronic Obstructive Pulmonary Disease Patients
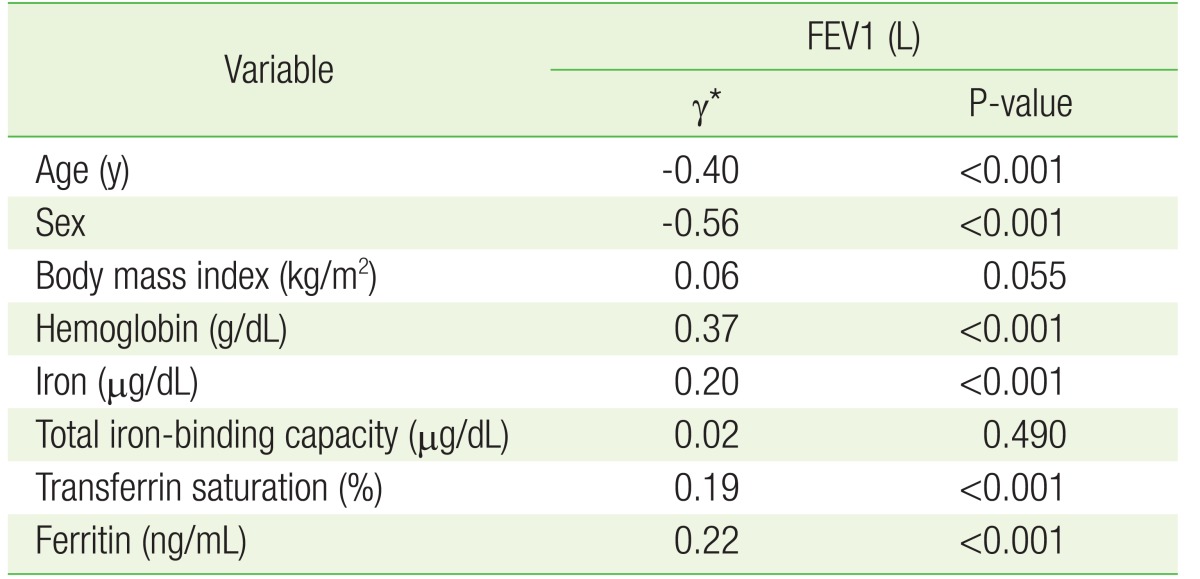
Table 2 shows the Spearman correlation analyses between FEV1 and the other variables, including Hb and iron parameters, in patients with COPD. The FEV1 was positively correlated with serum Hb (╬│=0.37, P<0.001), iron (╬│=0.20, P<0.001), TSAT (╬│=0.19, P<0.001), and ferritin (╬│=0.22, P<0.001), and negatively correlated with age (╬│=ŌłÆ0.40, P<0.001) and lower in female patients (╬│=ŌłÆ0.56, P<0.001).
3. Relationships of FEV1 with Hemoglobin and Iron Parameters in Chronic Obstructive Pulmonary Disease Patients
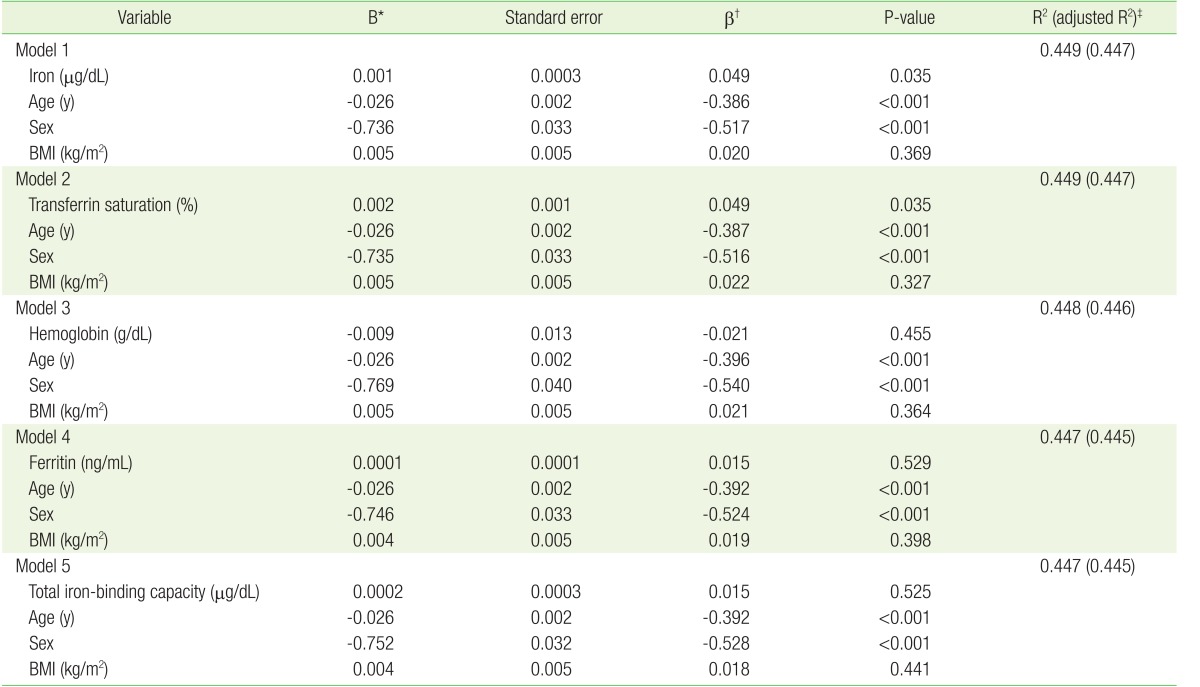
Table 3 shows the multiple linear regression analyses between FEV1 and the variables, including serum Hb and iron parameters (iron, TIBC, TSAT, and ferritin), after adjustment for age, sex, and BMI. The multiple linear regression revealed serum iron (╬▓=0.049, P=0.035) and TSAT (╬▓=0.049, P=0.035) were independent determinants of FEV1 as an indicator of lung function after adjustment for age, sex, and BMI (models 1 and 2). Although the levels of Hb, ferritin, and TIBC significantly correlated with FEV1 in the Spearman correlation analyses (Table 2), they did not correlate with FEV1 after adjustment for age, sex, and BMI in the multiple linear regression analyses (Table 3: models 3, 4, and 5).
DISCUSSION
In this nationwide study, the serum iron and TSAT levels were found to be positively related with the FEV1 as an indicator of COPD severity after adjustment for age, sex, and BMI; that is, serum iron and TSAT negatively correlated with the severity of COPD. This finding indicates that the serum iron and TSAT levels could represent biomarkers of COPD severity.
In this study, absolute FEV1 was used to represent the severity of COPD and lung function instead of predicted FEV1. The severity of airflow limitation in COPD is stratified by the percentage of the predicted FEV1 in the GOLD classification.8) However, application of the predicted FEV1 levels may lead to inappropriate assessments of severity across different ethnicities, age groups, and sexes. Although patients may have the same absolute FEV1 levels, they may be categorized into different COPD severity levels depending on the reference equations.9) Miller and Pedersen10) found that using absolute FEV1 levels could better predict the survival rate compared with the predicted FEV1 values. Based on our results herein, the serum iron and transferrin saturation levels could be considered as biomarkers to support lung function as assessed by FEV1 in COPD patients.
This present study revealed that serum iron and TSAT were associated with FEV1 after adjustment for age, sex, and BMI in COPD patients using nationwide data. In a previous study, iron status was found to be associated with lung function and disease progression in COPD, with lower serum iron and TSAT associated with elevated mortality in patients with chronic respiratory failure. In addition, the authors also found that TSAT and Hb were independently associated with dyspnea.11) Another study showed that reduced iron intake was related with an increased risk of COPD and decreased percentage of the predicted FEV1, though the correlation coefficients were low.12)
In this study, low serum iron and TSAT were related with severe COPD. COPD represents a generalized inflammatory status with elevated production of acute-phase proteins, such as ferritin and hepcidin, and inhibited iron mobilization from reticuloendothelial iron stores, which could result in a functional iron deficiency (ID) despite high ferritin levels. Currently, a ferritin cut-off level of <12 ng/mL is considered to have a very high specificity for the prediction of absolute ID;13) however, the criterion for anemia should be different in patients with COPD compared with that in healthy individuals, because the pathogenesis of COPD involves a combination of inflammation, hypoxemia, and ID. Thus, because there are currently no definite clinical Hb or iron parameter cut-off levels for detecting anemia among COPD patients, further studies are needed.
Several studies have shown that the treatment of anemia or ID should be considered in COPD patients. Non-anemic ID was found to be related to decreased aerobic capacity and a lower pulmonary rehabilitation response in COPD patients compared with in patients with normal iron status in one previous study.14) Further, some studies have shown the benefits of iron supplementation in chronic inflammatory disease states such as COPD, congestive heart failure, and chronic kidney disease. Indeed, intravenous iron treatment has been shown to improve functional capacity and quality-of-life in chronic kidney disease15) and heart failure patients with ID, either with or without anemia.16,17) Furthermore, Silverberg et al.18) suggested that dyspnea in COPD patients may be improved with the use of erythropoiesis-stimulating agents and intravenous iron to correct for ID.
Serum iron and TSAT have several advantages as biomarkers in COPD, including cost-effectiveness, simplicity, their significant relationship with FEV1, and relationship with the treatment. Nevertheless, before routinely using iron supplementation as a treatment, further studies should be conducted to examine the risks and effects of iron overload toxicity and the appropriate amount of iron for the treatment of ID in COPD patients. Further, the fact that polycythemia can lead to pulmonary hypertension and venous thromboembolism should be considered.19)
There were some limitations to the present study. Because the KNHANES V did not collect data on the C-reactive protein levels, we were inevitably not able to exclude subjects with elevated C-reactive protein levels, which indicate an acute inflammatory state. To resolve this limitation, we excluded subjects with elevated white blood cell levels as a marker of the inflammation state. Another major limitation is the fact that reversibility tests using bronchodilators were not performed, hence resulting in potential overlap with asthma. However, chronic asthma may also demonstrate traits of irreversible airflow obstruction and thus be included in the definition of ŌĆ£COPD.ŌĆØ20)
In conclusion, the serum iron (╬▓=0.049, P=0.035) and TSAT (╬▓=0.049, P=0.035) levels were independently associated with FEV1 as a marker of COPD severity.