Validity and Reliability of Korean Version of International Physical Activity Questionnaire Short Form in the Elderly
Article information
Abstract
Background
Estimation of physical activity contributes to early screening and prevention of decrease in body function. This study was conducted to examine the reliability and validity of the International Physical Activity Questionnaire (IPAQ) short form in elderly people.
Methods
A total of 55 outpatients of 65 years old or older participated in this study. Physical activity over the last seven days was recorded on the IPAQ short form. Responses were converted to metabolic equivalent task minutes per week. The IPAQ short form was validated against accelerometer measurements as a gold standard. The test-retest method was performed over a two-week interval to examine the reliability of the IPAQ.
Results
The more physically active by the IPAQ short form, the higher the measured value of the accelerometer (P < 0.001). Pearson's correlation coefficient was 0.43 for the correlation between the results of two measurements. Spearman Rho coefficients and Kappa values of test-retest reliability in five elements (vigorous days, vigorous minutes, moderate days, moderate minutes, and walk days) were 0.299-0.605 and 0.307-0.418, respectively.
Conclusion
The validity of the IPAQ short form was proven, but the reliability was found to be low. Nevertheless, IPAQ short form seems worthwhile tool for the measurement of physical activity levels, concerning daily variation in physical activity of the elderly.
INTRODUCTION
Physical activity and regular exercise contribute to general health and mental well-being and are associated with reduced mortality.1,2) On the other hand, prolonged sitting is associated with an increased risk of all-cause mortality, cardiovascular disease risk,3) weight gain4) or obesity,5) metabolic syndrome,6) type 2 diabetes,5) and colon cancer.7) Nevertheless, physical inactivity and prolonged sedentary lifestyles have gradually increased. Moreover, most of the elderly experience functional limitations and impairments that lead to a decrease in physical activity. A variety of studies have reported that physical activity and regular exercise for in the elderly have played an important role in improving quality of life8) and slowing the gradual decline of bodily systems.9)
Until now, much attention has been paid on developing reliable and valid instruments to estimate activity levels and to measure the impact of intervention to promote physical activity.10) The benefit in estimating physical activity is that it allows for early screening and prevention of decrease. Various tools for measuring physical activity include motion sensors such as pedometers and accelerometers or heart rate monitors, etc.11,12)
But the preferred methods of measurement may not always be feasible to use because of cost and inconvenience. On the contrary, a simple and reliable questionnaire would have the advantages of low cost, convenience, and ease of various data collection. Self-reported questionnaires for measuring physical activity of the general population include the Health Insurance Plan of New York Activity Questionnaire,13) the Baecke Questionnaire of Habitual Physical Activity,14) the Lipid Research Clinics Questionnaire,15) the Kuopio Ischaemic Heart Disease Risk Factor 24-hour Total Physical Activity Record,16) and the Aerobic Center Longitudinal Study Physical Activity Questionnaire.17)
Of the many published questionnaires, the International Physical Activity Questionnaire (IPAQ) has been investigated and used in many populations. The IPAQ was developed by the World Health Organization in 1998 (http://www.ipaq.ki.se) for surveillance of physical activity and to facilitate global comparison. The IPAQ questions are adapted to cultural diversity, and use country-specific examples to help define physical activity and sitting. The 27-item long form and 7-item short form assess time spent on various activities. The 2 forms have been validated against accelerometer measurements as a gold standard in 12 countries. The short form is preferred by many researchers because it has equivalent psychometric properties to the long form.
The Korean version of IPAQ developed by Oh et al.18) was recognized as a valid tool for physical activity assessment. Oh et al.18) proved the reliability and the validity of the IPAQ short form. However, this study was examined for the subjects aged 15-69 and this report still lacks such confirmation in the elderly. The purpose of this analysis was to examine the reliability and the validity of the IPAQ short form in elderly people.
METHODS
1. Study Participants
From March 2011 to June 2011, a total of 55 outpatients of 65 years or older who visited senior welfare centers located in Seoul participated in this study. The subjects who could understand the self-reported questionnaire and fill in the questionnaire exactly were included. When the subjects had difficulty with reading because of low educational level or visual impairment, surveyors asked the subjects the questionnaire and filled in the questionnaire in place of them. For measurement of physical activity, the elderly in this study were confined to those who could stand and walk over 10 meters for themselves without any difficulties. Those with known Parkinson's disease, cerebrovascular disease or dementia (a mini-mental state examination-Korean version score under 18) and those who were taking anti-dementia drugs or anti-anxiety drugs, etc. were excluded in this study.
This study was approved by the Institutional Review Board of Sungshin Women's University, in Seoul, Korea (sswuirb201-005). The written consent was obtained from each patient before enrollment in the study.
2. Measurements and Methods
All participants were surveyed by one trained surveyor with a structured questionnaire and screening tools for depression, impaired cognitive function and other disabilities and impairments.
1) Demographic characteristics
Participants were asked age, sex, education level, economic status, living arrangement, alcoholic consumption, and smoking. Education status was divided into none, elementary school, middle school, high school, and university. Family income was divided into "<0.5," "0.5-1," "1-1.9," "2-3.9," and "≥4 million won per month." Living arrangement was divided into "elderly alone," "elderly with spouse," "elderly with offspring," and "other." Presence or absence of chronic illness was asked. Major chronic illnesses were grouped as diabetes mellitus, hypertension, osteoarthritis, cancer, and others. Height, weight, and blood pressure were measured.
2) International physical activity questionnaire
Short form of IPAQ recorded physical activity in the last seven days. The 7-items of IPAQ identified the total minutes over the last seven days spent on moderate and vigorous-intensity physical activity, walking physical activity, and inactivity. To examine the reliability of the IPAQ, the test-retest method was performed over a two-week interval. Responses were converted to metabolic equivalent task minutes per week (MET-min/wk) according to the IPAQ scoring protocol.10) Using the Ainsworth et al.19) compendium, an average MET score was derived for each type of activity. The following values continued to be used for the analysis of IPAQ data: walking = 3.3 METs, moderate physical activity = 4.0 METs, vigorous physical activity = 8.0 METs, and total physical activity MET-min/wk = sum of walking + moderate + vigorous MET-min/wk scores.
In addition, physical activities were categorized as low, moderate, and high level of physical activity.18) Low physical activity: no activity or some activity but not enough to fall under categories 2 or 3. Moderate physical activity: either of the following 3 criteria (3 or more days of vigorous activity of at least 20 minutes per day, 5 or more days of moderate-intensity activity and/or walking of at least 30 minutes per day, 5 or more days of any combination of walking, moderate-intensity or vigorous-intensity activities achieving a minimum of at least 600 MET-min/wk). High physical activity: any one of the following 2 criteria (vigorous-intensity activity for at least 3 days and accumulating at least 1,500 MET-min/wk, 7 or more days of any combination of walking, moderate- or vigorous-intensity activities accumulating at least 3,000 MET-min/wk) (http://www.ipaq.ki.se).
3) Accelerometer
The IPAQ short form was validated against accelerometer (Lifecorder; Suzuken Co. Ltd., Nagoya, Japan) measurements as the gold standard in this study. The Lifecorder is widely used as an objective measurement of physical activity and reported to be correlated with other accelerometers.20) The Lifecorder is an uni-axial accelerometer and it measures acceleration in the vertical direction. Participants wore the Lifecorder around the waist during three consecutive days for all waking hours, removing it only for bathing or sleeping.
According to technical details provided by the manufacturer (Suzuken Co. Ltd.), the accelerometer samples the acceleration at 32 Hz and assesses values ranging from 0.06 to 1.94 g. A maximum pulse over 4 seconds is taken as the acceleration value, and the activities are categorized into eleven activity levels (0, 0.5, 1.0-9.0) based on the pattern of the accelerometric signal. The activity levels are subsequently converted by an algorithm to calculate energy expenditure (kcal).
3. Statistical Analysis
Descriptive data were expressed as the mean ± SD or percentage. A post hoc test in ANOVA was used to determine specific differences between the three levels of physical activity. Pearson's correlations were used to determine the correlation between the measurements. Spearman's correlation and Kappa values were performed to determine test-retest reliability of the IPAQ short form. For analysis of Kappa values, some items of IPAQ were categorized. Vigorous activity time was categorized into 0-19 minutes, 20-59 minutes, 60 minutes, and over. Likewise, moderate activity time and walking was categorized into 0-29 minutes, 30-59 minutes, 60 minutes, and over. Sitting time was categorized into 0-119 minutes, 120-359 minutes, 360 minutes, and over. The number of days of physical activity during the last week was categorized into 0, 1-3 days, 4-6 days, and 7 days.
All statistical results were based on two-sided tests. Significance was accepted at the P < 0.05 level. Data were analyzed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. General Characteristics of the Study Populations
Baseline characteristics of the study subjects are displayed in Table 1. The mean age of the subjects for both women and men was 75.2 ± 5.3 years. The proportion of the subjects who are living alone (15.0% in men, 34.3% in women) and with spouse only (70.0% in men, 42.9% in women) were higher than the subjects with off spring in both men and women (15.0% in men, 20.0% in women). The proportion of subjects who have low family income (under 0.5 million won/mo) was higher than that of other groups (25.0% in men, 48.6% in women).
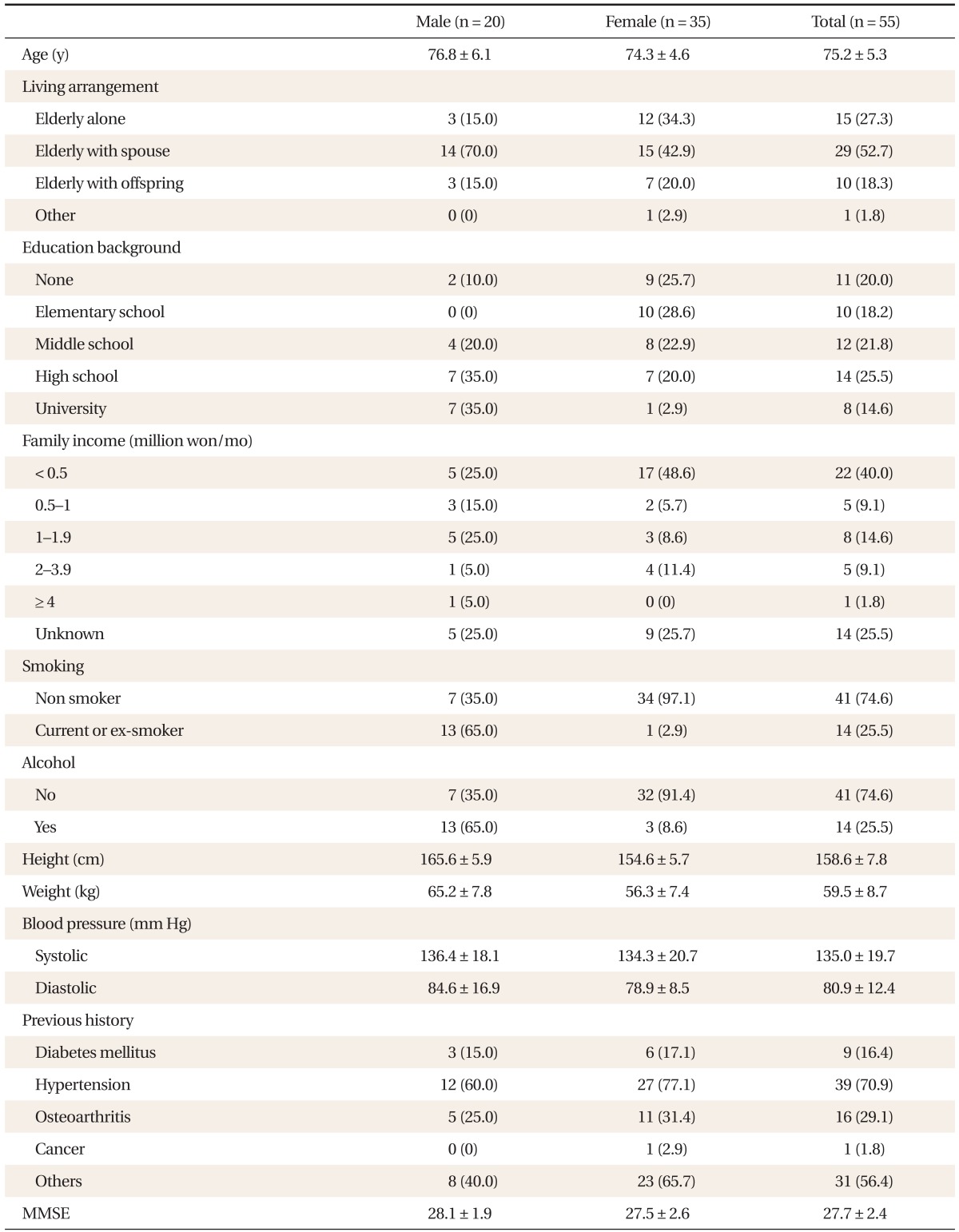
General characteristics of the study subjects.
2. Comparison of Energy Expenditure Measured by Accelerometer between the Three Levels of Physical Activity
Physical activity was categorized according to IPAQ classification and analyzed to examine the difference in energy expenditure measured by the accelerometer in Table 2. The number of subjects with low physical activity was 14, that of moderate physical activity was 21, and that of high physical activity was 20. The self-reported energy expenditure (MET-min/wk) in the high activity group was significantly greater than that of low and moderate activity groups (6,461.18 ± 3,474.53 MET-min/wk in high activity group vs. 1,581.19 ± 620.28 MET-min/wk in moderate activity group, and 288.15 ± 191.09 MET-min/wk in low activity group; P < 0.001). Energy expenditure for 3 days measured by accelerometers in the low activity group was lower than the energy expenditure in the moderate and high activity groups (P = 0.009).

Comparison of energy expenditure measured by accelerometer between the three levels of physical activity according to the IPAQ short form.
3. Correlation between the Result of the IPAQ Short Form and Energy Expenditure Measured by Accelerometer
Table 3 shows the correlation between IPAQ-reported energy expenditure (MET-min/wk) and energy expenditure measured by accelerometer. The more physically active by the IPAQ short form, the higher the measured value of the accelerometer (P < 0.001). Pearson's correlation coefficient was 0.43 for the correlation between the results of the two measurements.

Correlation between the result of the IPAQ short form and energy expenditure measured by accelerometer.
4. Test-Retest Reliability of the Short Form IPAQ
Table 4 shows test-retest reliability of the short form IPAQ over a two-week interval. Spearman Rho coefficients and Kappa values of test-retest reliability in five elements (vigorous days, vigorous minutes, moderate days, moderate minutes, and walking days) were 0.299-0.605 and 0.307-0.418, respectively. But two elements of IPAQ (walking minutes and sitting minutes) were not significant.
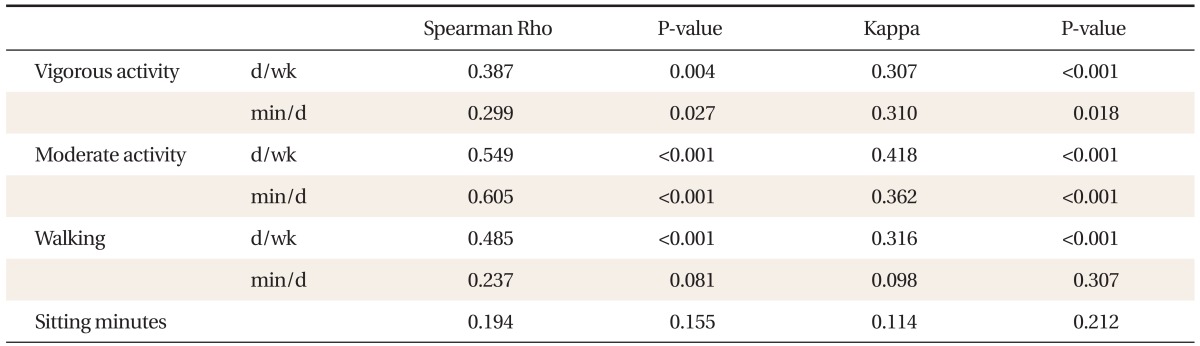
Test-retest reliability of the short form IPAQ.
DISCUSSION
The decline in physical activity has important public health implications for older people, since there is increasing evidence that health effects of physical activity are linked specifically to the total amount of kilocalorie expenditure of activity time.20) The new Centers for Disease Control and Prevention/American College of Sports Medicine recommendations are especially useful for older people as they emphasize the value of moderate-intensity activity as well as the daily accumulations of physical activity. Thus the recommended accumulated expenditure of 200 kcal/d can be achieved easily by most older people through short bouts of activity such as stair climbing, gardening, walking, and playing with children or doing housework.21) To apply these recommendations as a part of daily lifestyle, we need to measure the energy expenditure of physical activity first.
There have been many developments in physical activity questionnaires as simple and feasible measurements for the elderly such as the Modified Baecke Quesionnaire for older adults,22) the Zutphen Physical Activity Questionnaire,23) the Physical Activity Scale for the Elderly,24) the activity of daily living, the instrumental activity of daily living, and the Yale Physical Activity Survey.
But there are few physical activity questionnaires reflecting characteristics of physical activity in Korean elderly people. It may be most appropriate to use the existing questionnaires in Korea as well. However, their reliability must first be validated in older age groups.
Choe et al.25) developed a Korean version of the Physical Activity Scale for the Elderly (K-PASE) and reported K-PASE was a reliable and valid instrument to assess physical activity in Korean elderly. In this report, validity was established by correlating the K-PASE scores between the Tokyo Metropolitan Institute of Gerontology index of competence and hand-grip strength. However the Pearson's correlation coefficients were low.
The IPAQ has been recommended and widely used as a surveillance instrument but there have been arguments about its validity when comparing its measurements to objective measurements of physical activity.26,27) Oh et al.18) also reported the reliability and validity of the IPAQ short form in Korean people but the correlations were lower than that of other health variables. Spearman Rho coefficient was 0.267 for the correlation between the results of the questionnaire and measured values by accelerometer. The Spearman Rho coefficients and Kappa values of test-retest reliability were 0.427-0.646 and 0.365-0.620, respectively.18) Although IPAQ had low correlations with the objective measurements, the IPAQ is one of the easiest of physical activity questionnaires to administer with less than 10 questions. Given the advantages of IPAQ, including its ease of administration and low cost, it seems worthwhile to use as a measurement of physical activity.
The IPAQ Korean version has been also used for the elderly. Park28) identified the relationship between physical activity measured by the IPAQ and sleep patterns of Korean elderly. Seo et al.29) suggested that physical activity measured by the IPAQ may be associated with cognitive function.
This cross-sectional study of elderly people in Seoul, Korea was performed to investigate the reliability and validity of the IPAQ short form. The IPAQ short form was validated against uni-axial accelerometer measurements as a gold standard. Although the uni-axial accelerometer underestimated the total daily energy expenditure, the energy expenditure measured by this showed correlation with other objective measurements.20) The correlation between two measurements was positively significant (Pearson's correlation coefficient, 0.43; P < 0.001). And the consistency of test and retest in five elements of IPAQ (vigorous days, vigorous minutes, moderate days, moderate minutes, and walking days) was fair to moderate. Two elements of IPAQ (walking minutes and sitting minutes) were not reliable. This low reliability may be caused by considerable daily variation according to health conditions in the elderly.
There were several limitations in this study. These data are likely to apply to individuals of low socioeconomic status who live in the city. They may have difficulty providing valid physical activity data, and data were more likely to be missing from those who lived in the country and had vigorous physical activity. A further limitation was the use of the accelerometer, as there may have been missing data of energy expenditure caused by measuring only uni-axial physical activity and inconvenience of wearing. The previous study showed that total energy expenditure measured by uni-axial accelerometer was significantly underestimated by a mean value of 8%. However, a highly significant relationship was demonstrated between the measured values by uni-axial accelerometer and those in the respiratory chamber.20)
In conclusion, the validity of the IPAQ short form was demonstrated. However, the reliability was found to be low. Nevertheless, the IPAQ short form seems worthwhile to use as a tool for measuring physical activity levels in the elderly.
ACKNOWLEDGMENTS
This work was supported by a grant from Sungshin Women's University.
Notes
No potential conflict of interest relevant to this article was reported.