INTRODUCTION
Metabolic syndrome is known to be an important risk factor for type II diabetes and cardiovascular diseases, in which its presence increases the mortality rate.1-3) The risk of metabolic syndrome was reported to increase with the occurrence of heavy consumption of alcohol.4) Although moderate drinkers showed less risk of metabolic syndrome than heavy drinkers, various other risks of metabolic syndrome were observed compared to the non-alcohol consuming group. Urashima et al.5) reported a higher risk of metabolic syndrome in moderate drinkers compared to non-drinkers, but Wakabayashi reported a contrary result of reduced atherosclerotic risk in moderate drinkers.6)
The occurrence of facial flushing is the typical hypersensitivity symptom of alcohol consumption, which occurs by a temporary increase of blood suppy to facial skin when facial blood vessels dilate. Within the human body, alcohol is broken down to acetaldehyde by the action of alcohol dehydrogenase, and then metabolized as acetate by aldehyde dehydrogenase (ALDH). The acetaldehyde intermediate that is produed during metabolism is related to the occurrence of facial flushing.7) An alcohol drinker showing facial flushing from deficiency of the ALDH2 enzyme tends to remain in a metabolically heavy drinking status, even if the alcohol consumption was moderate. In the case of showing facial flushing under the same alcohol drinking condition, the risk of metabolic syndrome can be observed in a different pattern. However, it is difficult to find studies that discuss the risk of metabolic syndrome according to the amount of alcohol consumption in drinkers with facial flushing. Therefore, the authors of the present study evaluated the risk of metabolic syndrome according to alcohol consumption for those subjects showing facial flushing, as well as those without facial flushing.
METHODS
1. Subjects
The present study selected all 1,323 male outpatients who visited a health promotion center in Chungnam National University Hospital from January to June, 2009. Among them, the present study was performed by subjecting 1,201 patients, excluding the patients without medical records on past history of diseases such as hypertension, diabetes and dyslipidemia, alcohol drinking amount, smoking, exercise amount, and occurrence of flushing at the time of alcohol drinking, along with patients who did not respond to the questionnaire.
2. Methods
Through patient interview and questionnaire, alcohol consumption amount, smoking, exercise amount, and the occurence of facial flushing were evaluated. Weekly standard drinks (one standard drink is equal to 14 g of alcohol) were estimated after evaluating alcohol drinking amount at a single sitting (in bottles) and alcohol drinking frequency per week. According to the criteria of the US National Institute on Alcohol Abuse and Alcoholism, the alcohol drinking group consuming 14 standard drinks or less, and those consuming more than 14 standard drinks were categorized as moderate drinkers and heavy drinkers, respectively. Smoking was divided into nonsmokers, ex-smokers, and smokers. Smokers were evaluated by their smoking amount (in packs) and by their smoking period (in years). Exercise amount was evaluated and categorized into non-exercising group, irregular-exercising group (exercising less than three times per week), and regular-exercising group (more than three times per week at 30 minutes or more each time). After evaluating the occurence frequency (always, occasional, no occurrence) of facial flushing at the time of alcohol consumption, the groups that always experienced facial flushing and the group without facial flushing were classified as flushers and non-flushers, respectively. The group that occassionally experienced facial flushing was excluded from evauation.
The body weight of subjects was measured to the nearest 0.01 kg unit by fitting them in medical examining outerwear. Height was measured on a 0.1 cm scale by using an automatic height measuring system. The body mass index (BMI) value was calculated by dividing body weight (kg) by squared height (in meters) and expressed as kg/m2. Waist circumference was measured at the straight upper part of the illiac crest to a 0.1 cm unit at the end of expiration by horizontally maintaining the illiac crest with the bottom. Upper arm blood pressure of resting subjects was measured by using an automatic blood pressure measuring device after stablilizing the test subjects for more than 10 minutes. Blood was collected after maintaining more than 12 hours of fasting to measure the levels of tirglyceride (TG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density cholesterol, and the fasting plasma glucose (FPG) level.
Based on the diagnostic criteria that was defined at the National Cholesterol Education Program-Adult Treatment Panel III, the subjects who satisfy more than three of following conditions were defined as patients with metabolic syndrome. The case of conducting drug therapy for hypertension, diabetes, and dyslipidemia was included in each comprising factor. The waist circumference for the diagnosis of abdominal obesity used in the criteria is that suggested for Asians by the World Health Organization.8)
The criteria for metabolic syndrome were as follows: waist circumference Ōēź 90 cm in male, triglyceride Ōēź 150 mg/dL, HDL-cholesterol Ōēż 40 mg/dL in male, blood pressure Ōēź 130/85 mm Hg and fasting plasma glucose: Ōēź 100 mg/dL.
3. Data Analysis
The subject group was initially divided into non-drinkers, moderate drinkers, and heavy drinkers, and both moderate and heavy drinkers were divided again as flushers and non-flushers. The characteristics of each group were analyzed by one-way analysis of variance and chi-square tests. To evaluate the risk of metabolic syndrome in both flushers and non-flushers against the non-drinkers, logistic regression analysis was performed after adjusting the confounding variables of age, exercise amount, smoking, and BMI. All statistical analysis was performed by using the SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA). The statistically significant P-value was set at 0.05.
RESULTS
1. Characteristics of Subjects
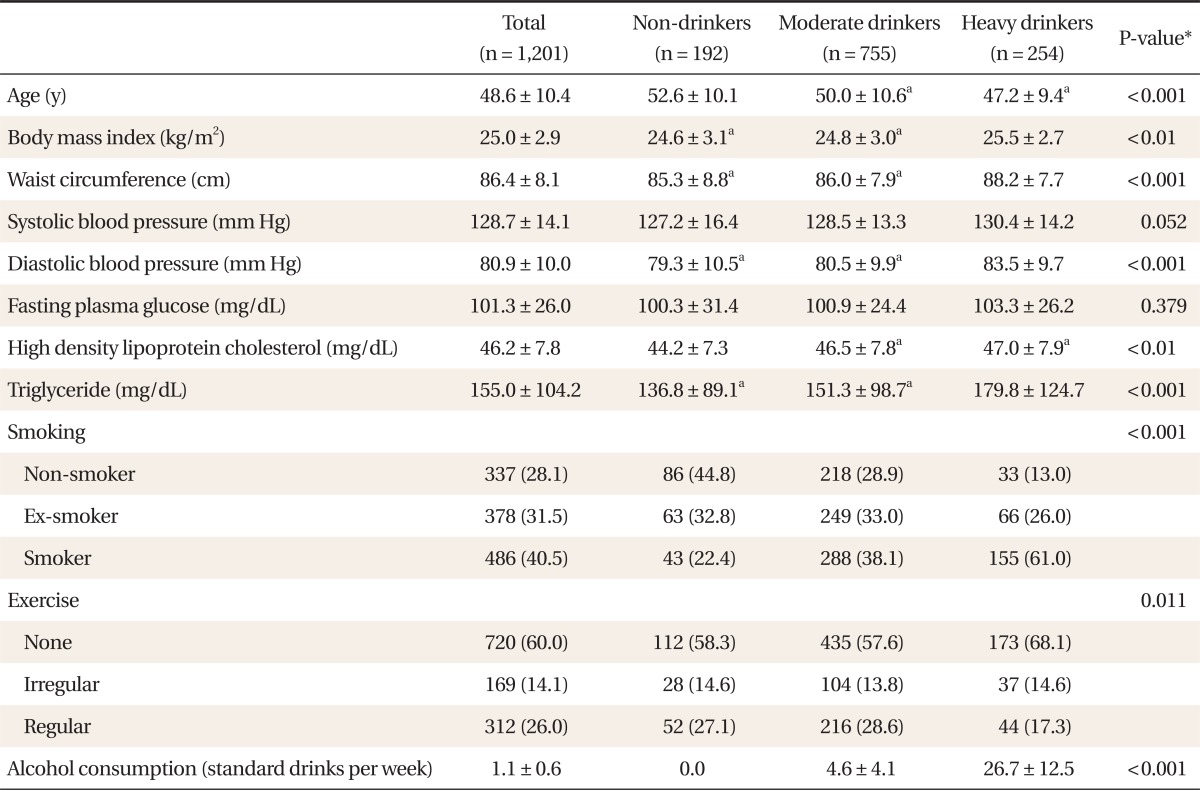
Among the 1,201 total subjects, 192 were included in the non-drinkers (16.0%), 775 subjects were included in the moderate drinkers (62.9%), and 254 subjects were included in the heavy drinkers (21.1%). The non-flusher ratio among total alcohol drinkers was 48.3% (487/1,009). Excluding the 227 subjects who occasionally experienced hot flushing at the time of alcohol consumption, 782 subjects were included in the alcohol consumption groups, with 487 subjects categorized into the non-flushers and 295 subjects categorized into flushers. The non-flushers included 340 moderate drinkers and 147 heavy drinkers. The flushers included 254 moderate drinkers and 41 heavy drinkers. The weekly average alcohol consumption amount of all subjects ranged around 1.10 (┬▒ 0.60) standard drinks, with moderate alcohol drinkers ranging at 4.6 (┬▒ 4.1) standard drinks, and heavy drinkers at 26.69 (┬▒ 12.52) standard drinks.
The mean age of non-drinkers was found to be significantly higher than that of moderate and heavy drinkers. BMI, waist circumference, diastolic blood pressure, and triglyceride level were significantly higher in the heavy drinkers than those of non-drinkers and moderate drinkers. No significant difference was observed in systolic blood pressure and fasting plasma glucose level. Among the heavy drinkers, the highest smoking ratio observed was 61.0%. The smoking ratio in the moderate drinkers showed approximately 38.1%, and the lowest smoking ratio of 22.4% was observed in the non-alcohol consuming group. The ratio of performing regular exercise more than three times a week in the moderate drinkers and non-drinkers recorded 28.6% and 27.1%, respectively, and the lowest exercise performance ratio of 17.3% was observed in heavy drinkers (Table 1).
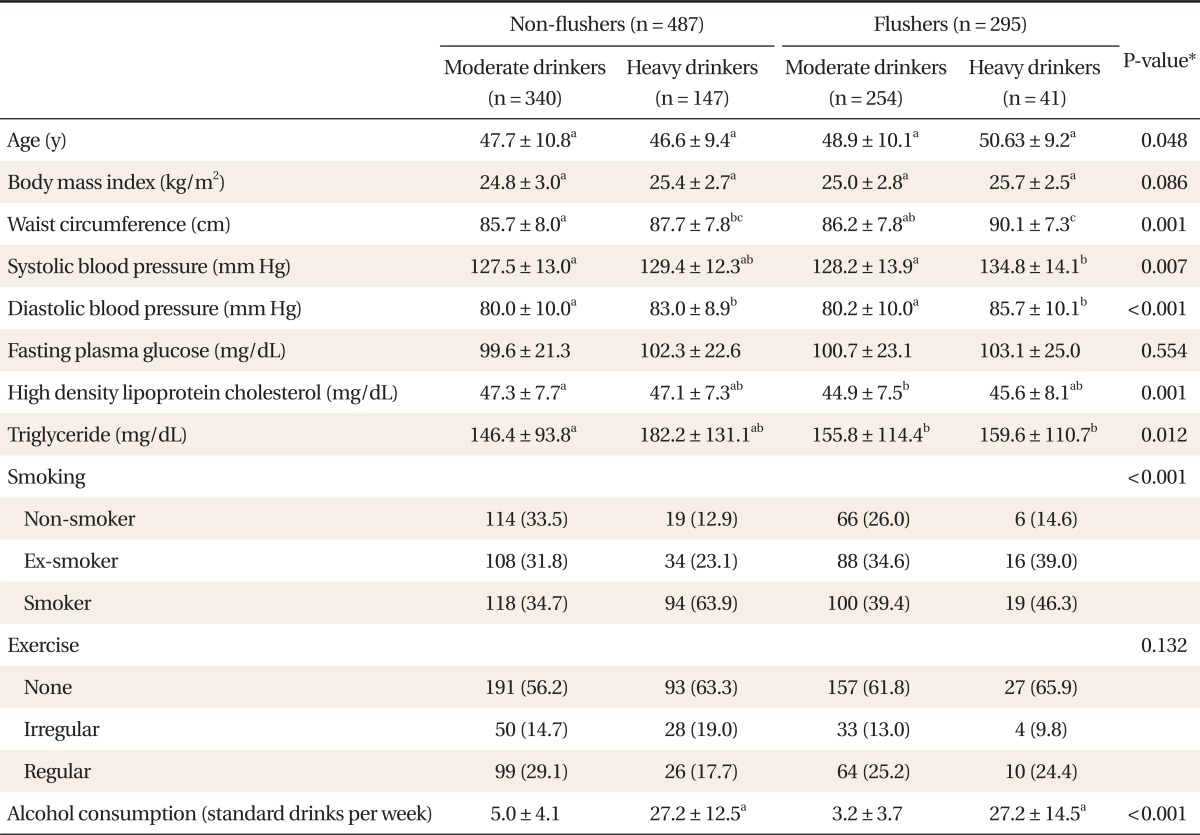
In both non-flushers and flushers, the waist circumference and diastolic blood pressure showed significantly higher values in heavy drinkers than moderate drinkers. Among the non-flushers, the systolic blood pressure of the heavy drinkers was significantly higher than that of moderate drinkers. The highest smoking ratio of 63.9% was observed in non-flushing heavy drinkers, followed by 46.3% in flushing heavy drinkers, 39.4% in flushing moderate drinkers, and the lowest smoking ratio of 34.7% in non-flushing moderate drinkers. When evaluating the regular exercise performance ratio of conducting exercise more than three times per week, the highest exercise performance ratio of 29.1% was observed in non-flushing moderate drinkers, followed by 25.2% in flushing moderate drinkers, 24.4% in flushing heavy drinkers, and 17.7% in non-flushing heavy drinkers, without showing a significant difference between the groups (Table 2).
2. Logistic Regression Analysis between Alcohol Consumption and Metabolic Syndrome by the Presence of Facial Flushing
Among all groups, the odds ratio (OR) of metabolic syndrome for the moderate drinkers against non-drinkers after adjusting the variables of age, exercise amount, and smoking status recorded 1.47 (95% confidence interval [CI], 0.94 to 2.31; P = 0.094), and that of the heavy drinkers recorded 2.40 (95% CI, 1.42 to 4.04; P = 0.001).
Among non-flushers, the OR of metabolic syndrome for the moderate drinkers against non-drinkers, after adjusting the variables of age, exercise amount, and smoking status recorded 1.19 (95% CI, 0.71 to 2.00; P = 0.508), and that of heavy drinkers recorded 2.23 (95% CI, 1.23 to 4.04; P = 0.008).
Among flushers, the OR of metabolic syndrome for moderate drinkers against non-drinkers, after adjusting the variables of age, exercise amount, and smoking status recorded 1.81 (95% CI, 1.08 to 3.06; P = 0.025), and that of the heavy drinkers recorded 2.90 (95% CI, 1.25 to 6.73; P = 0.013) (Table 3).
3. Relationship between Alcohol Consumption Amount and Metabolic Syndrome Components by the Presence of Facial Flushing
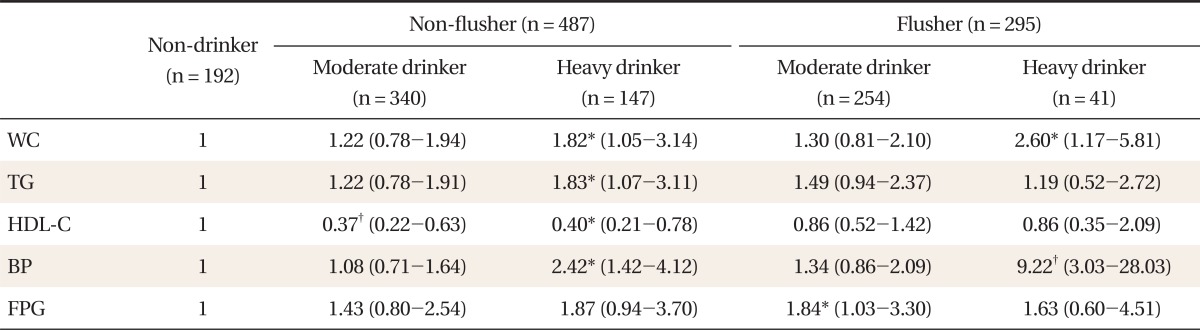
The OR of metabolic syndrome components against non-drinkers is represented in Table 4. The ORs of abdominal obesity for non-flushing and flushing heavy drinkers against non-drinkers showed a significant increase of 1.82 and 2.60, respectively. The OR of triglyceride increase was significantly higher in non-flushing heavy drinkers at 1.83. The OR of blood pressure increase was significantly higher in non-flushing and flushing heavy drinkers at 2.42 and 9.22, respectively. In particular, the OR of blood pressure increase in flushing heavy drinkers showed the highest OR value at 9.22, which display the highest OR value among the comprising factors of metabolic syndrome. The OR of FPG increase was significantly higher in flushing moderate drinkers at 1.84. The OR of HDL-C reduction was found to show a significant reduction of 0.37 and 0.40 in non-flushing moderate drinkers and non-flushing heavy drinkers, respectively (Table 4).
DISCUSSION
The present study evaluated the risk of metabolic syndrome according to the presence of facial flushing and alcohol consumption amount in males. Most previous studies reported a higher risk of metabolic syndrome in the heavy drinkers than moderate drinkers.6,9) However, the group with the lowest considered risk of metabolic syndrome could be either moderate drinkers or non-drinkers, depending upon the study results. Moreover, studies on the risk of alcohol related metabolic syndrome according to the presence of facial flushing are difficult to find.
ALDH is primarily divided into the two isozymes of ALDH1 and ALDH2, and the occurrence facial flushing from alcohol response can be easily developed by deficiency of ALDH2.10-12) A study reported that 50% of Asians who reside in the US showed facial flushing at the time of alcohol consumption.13) It was reported that 51.6% of normal Korean adults have an inactive form of the ALDH2 gene.14) Since facial flushing is frequently observed among Asians, it is often referred to as the 'Asian Flush'.15) The authors of the present study reported non-flushers ratio to be 48.3%, which is similar to the 51.6% ratio of inactive form of the ALDH2 gene that was suggested by Bang.14) Therefore, the facial flushing ratio in the present study could be similarly considered as the general facial flushing ratio of Koreans.
Based on the study analysis result of the 1998 Korean National Health and Nutrition Examination Survey, the group that drank less than 15 g of alcohol per day resulted to show lower risk of metabolic syndrome than the non-drinkers, but the risk of metabolic syndrome increased proportionally to the amount of alcohol consumption.16) In a study that was performed with Japanese subjects, the lowest risk of metabolic syndrome was observed in the group drinking less than 22 g of alcohol per day, but the group that consumed more than 44 g of alcohol per day revealed a significant increase compared to the non-alcohol consuming group.17) In a study that was performed with American subjects, the lowest risk of metabolic syndrome was observed in the group drinking 12.1 to 24 g of alcohol per day, and those consuming more alcohol than that amount showed a U-type increment of metabolic syndrome.18) Contrary to those results, the study that was performed with Korean subjects revealed no significant difference between the non-drinkers and moderate drinkers, but the risk was found to increase proportionally to alcohol consumption amount, showing a significant increase in the heavy drinkers (>30 g per day).9) In another study, the risk of metabolic syndrome was not significantly different between the non-drinkers and the group drinking less than 40 g of alcohol per day, but an increased risk in the heavy drinkers that drank more than 40 g of alcohol per day was reported. Most of the studies agree upon the increased risk of metabolic syndrome in heavy drinkers. However, the results on the group showing the lowest risk of metabolic syndrome were different between studies. In addition, most of the studies did not evaluate the risk of metabolic syndrome according to the presence of facial flushing. Similar to the study results of Lee et al.4) and Baik and Shin,9) the present study showed no significant difference in the risk of metabolic syndrome between the non-drinkers and moderate drinkers, but a significant increase of metabolic syndrome was observed in the heavy drinkers. If the risk was evaluated by the presence of facial flushing, non-flushers showed a significantly increased risk only in the heavy drinkers compared to non-drinkers; yet both moderate and heavy drinkers showed facial flushing with an increased risk of metabolic syndrome. The result could be explained by the study that reported more risk of developing coronary atherosclerosis caused by alcohol drinking in Type II diabetes patients with facial flushing than the patients without flushing,6) as well as the study that reported higher risk of developing high blood pressure in alcohol drinkers with facial flushing than without.19)
In the present study, even under a moderate alcohol consumption status, it was confirmed that the facial flushing group showed 1.8 times higher risk of having metabolic syndrome compared to the non-drinkers. Based on these results, moderate alcohol consumption can be risky if patients currently with metabolic syndrome or the patients with high risk of the syndrome encounter facial flushing everytime they engage in drinking alcohol. Since the present study is a cross sectional study, the direct clinical application of the study results have limitations. Therefore, it is considered necessary to perform further large scale prospective studies on moderate alcohol consumption amounts in subjects who experience hot flushing.
Among the comprising factors of metabolic syndrome, the risk of blood pressure increase showed a significant increase in both non-flushing and flushing heavy drinkers, and the OR was higher in flushers than non-flushers. Although the risk of HDL-C reduction was lower in non-flushing moderate and heavy drinkers than non-drinkers, both flushing moderate and heavy drinkers showed no significant differences. The study results seem similar to the previous study results that reported a higher risk of arteriosclerosis and high blood pressure in the hot flushing group compared to the non-hot flushing group.19,20)
The limitations of the present study are listed below. Firstly, since the present study is a cross sectional study, it is difficult to predict the development of metabolic syndrome only according to the presence of facial flushing. Secondly, it is difficult to suggest this as a representative study for all Koreans, since the study was performed by subjecting people who received a general health check up in Chungnam National University Hospital (as well as being gender specific). Thirdly, the included test subject numbers are small. However, the present study is considered to be meaningful in evaluating the risk of metabolic syndrome by the presence of facial flushing, which reflects the alcohol metabolism rather than observing the relationship to metabolic syndome according to alcohol consumption amount.
In conclusion, regardless of facial flushing, heavy drinkers showed an increase risk of metabolic syndrome compared to non-drinkers. Non-flushing moderate drinkers did not show an increased risk of metabolic syndrome compared to non-drinkers, but flushing moderate drinkers showed an increased risk of metabolic syndrome compared to non-drinkers.