Effects of BATHE Interview Protocol on Patient Satisfaction
Article information
Abstract
Background
BATHE, the acronym for background, affect, trouble, handling, and empathy, is an interview approach that can be applied in the out-patient setting whereby questions belonging to each of the 5 categories are asked in the above order. As we have been taught to believe that BATHE raises the level of patient satisfaction and the quality of medical treatment overall, this study was designed to test the validity of the claim that applying BATHE heightens patient satisfaction.
Methods
Each of the 5 doctors was assigned 10 patients (5 in the BATHE group and the other 5 in the control group) with each patient being randomly assigned to either of the groups. The control group was interviewed as usual and the BATHE group was interviewed using BATHE. Immediately after the interview, each patient anonymously filled out a patient satisfaction questionnaire. Whether the questions asked were appropriate for each category of the protocol was evaluated by the researcher through video clips taped during the interviews.
Results
On 7 out of 10 items on the patient satisfaction questionnaire, the BATHE group was found to experience higher level of satisfaction than the control group in a statistically significant manner. The questions asked the BATHE group were confirmed to be more appropriate for each category of the protocol except empathy than those asked the control group.
Conclusion
As applying the BATHE approach was found to achieve higher level of patient satisfaction, we recommend using it in the out-patient setting.
INTRODUCTION
BATHE, the acronym for background, affect, trouble, handling, and empathy, was created to help the interviewer remember with ease the essentials of interview in outpatient settings. BATHE, the interview approach, was developed by Stuart and Lieberman1) to facilitate the evaluation of psychosocial factors pertaining to the patient's somatic complaint within 15 minutes of the outpatient appointment. Through BATHE, questions belonging to each of the 5 categories are asked in order, making it easier for the interviewer to express empathy and provide emotional support.
According to the literature to date, BATHE has been known for its ability to raise the quality of medical treatment and the level of patient satisfaction.2-4) As BATHE helps the patient clearly identify the basic questions of his life, right after the interview, the patient immediately feels better as he feels more in charge of his life. Empathic reaction and the interest extended by the doctor enables her to build rapport with the patient. Moreover, as the doctor is given the opportunity to demonstrate she is in charge of the patient's problem, the patient feels assured that his problem will be solved.5)
There have been only a small number of international studies done to examine the association between BATHE and the level of patient satisfaction. In one such study, designed to test the validity of the claim that applying BATHE heightens patient satisfaction, Leiblum et al.6) confirmed the group interviewed using BATHE reported greater satisfaction overall than the control group. So far, there has been no national study conducted to examine the association between BATHE and patient satisfaction or quality of medical care.
Hence, the aim of this study was to investigate the difference in the degree of patient satisfaction between the BATHE group and the control group, by having the patients visiting a family medicine outpatient clinic fill out a patient satisfaction questionnaire.
METHODS
1. Subjects and Methods
The study was conducted from July 4, 2011 through August 1, 2011 at Dankook University Hospital Family Medicine Outpatient Clinic. The researchers explained the purpose of this study and acquired informed consent from the participating doctors and the patients who came for outpatient visits.
The participating doctors were five family medicine residents at Dankook University Hospital (three men and two women). They received lessons on BATHE before the study. Moreover, they had ready access to BATHE during the interview; the standardized questions were typed and taped to the doctor's desk enabling them to ask the right questions at the right time. The specific questions belonging to each of the five categories of BATHE are shown in Table 1.
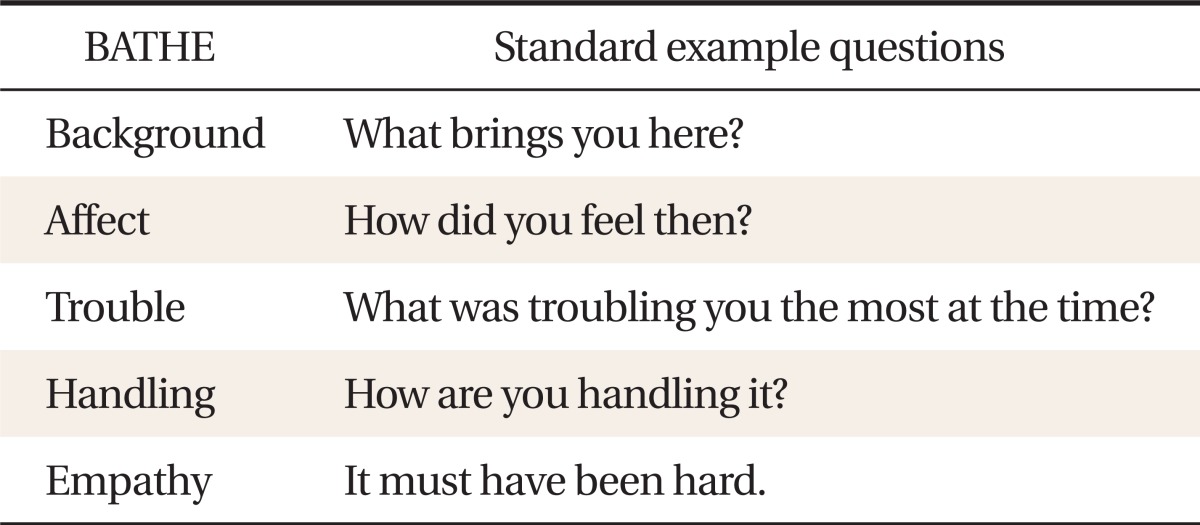
Examples of questions for background, affect, trouble, handling, and empathy (BATHE).
The study was conducted in two rounds. In the first round, each of the 5 doctors was assigned 5 patients in the order they came to the clinic. The doctors interviewed the patients as usual, not applying any systematic approach but employing empathy as usual. In the second round, 5 other patients were randomly assigned to each doctor in the same manner. The doctors, after gleaning information pertaining to the patient's present illness, applied the BATHE protocol.
Immediately after the interview, each patient filled out a patient satisfaction questionnaire anonymously. The questionnaire was based on the Calgary-Cambridge Medical Interview Guidelines and consisted of a total of 10 questions: attentiveness (2), good therapeutic alliance [rapport] (1), nonverbal communication (1), attitude (2), explanation (1), trust (1), length of interview (1), and overall satisfaction (1). Most of the patients completed the questionnaire within five minutes. Whether the doctors applied the BATHE protocol in appropriate fashion was evaluated by reviewing the video clips captured during the interviews through the cameras installed in the outpatient clinic.
2. Statistical Analysis
For comparison of categorical variables, Pearson chi-square test and Fisher's exact test were performed. Mann-Whitney U-test was performed in order to compare the satisfaction score of each item on the questionnaire and the overall satisfaction score between the BATHE group and the control group. The statistical significance was set at α = 0.05 and the data were analyzed using SPSS ver. 18 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Demographical Characteristics of Study Population
The study included a total of 50 patients. Twenty-seven (54%) of them were male, and 23 (46%) were female. The number of subjects belonging to each age group differed; 10 (20%) were in their twenties, 12 (24%) in their thirties, 7 (14%) in their forties, 10 (20%) in their fifties, and 11 in their sixties or over. The age of the subjects ranged from 20 to 72 with the mean age being 43.5 (± 15.4) years. In terms of age and sex, there was no statistically significant difference between the BATHE group and the control group (age, P = 0.31; sex, P = 0.19) (Table 2). Likewise, between the BATHE group and the control group assigned to each doctor, with regards to age and sex, there was no statistically significant difference (age, P = 0.68; sex, P = 0.26) (Table 3).
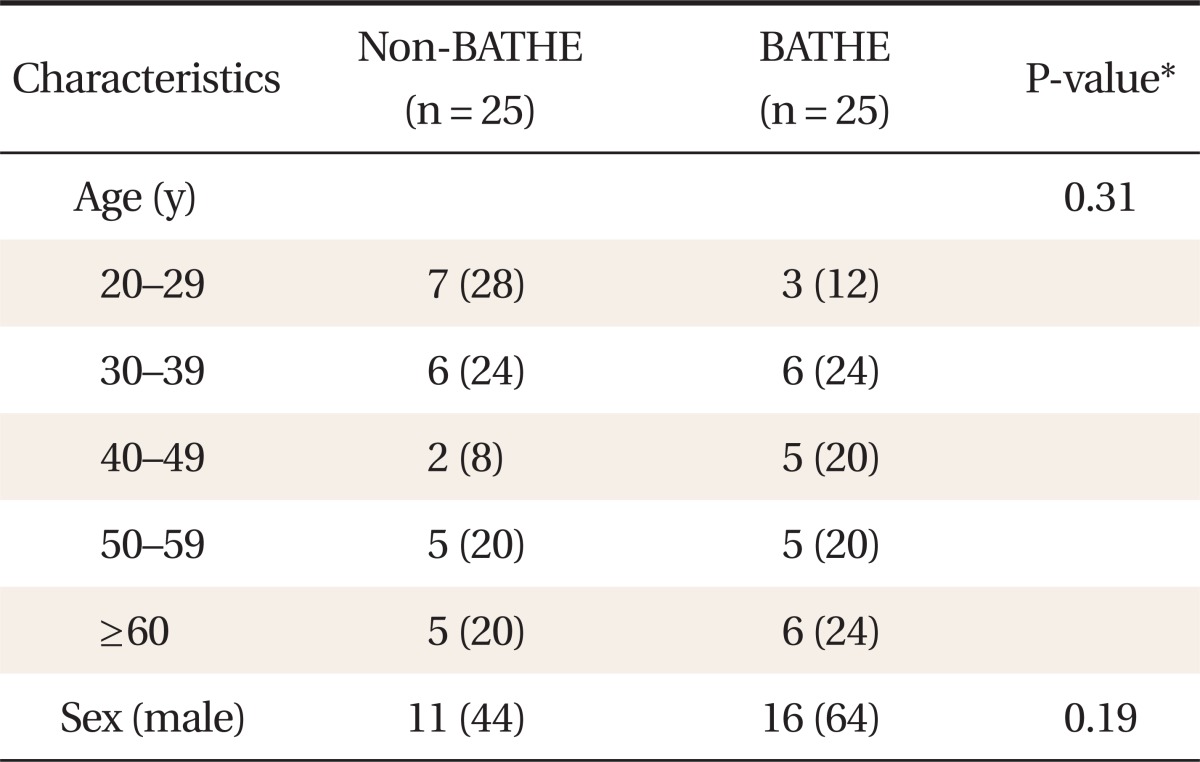
Demographic characteristics of the study population.

Demographic characteristics of the study population for each physician.
2. Application of the BATHE Interview Approach
Questions belonging to all of the five categories of BATHE excluding empathy were found to be asked more frequently to the BATHE group than the control group in a statistically significant manner. The percentage of subjects who thought their doctor expressed empathy during the interview was relatively high in both groups: 96% in the BATHE group and 76% in the control group. Although a greater percentage of subjects interviewed using BATHE recognized their interviewer's application of empathy, the difference between the two groups was not statistically significant (P = 0.42) (Table 4).
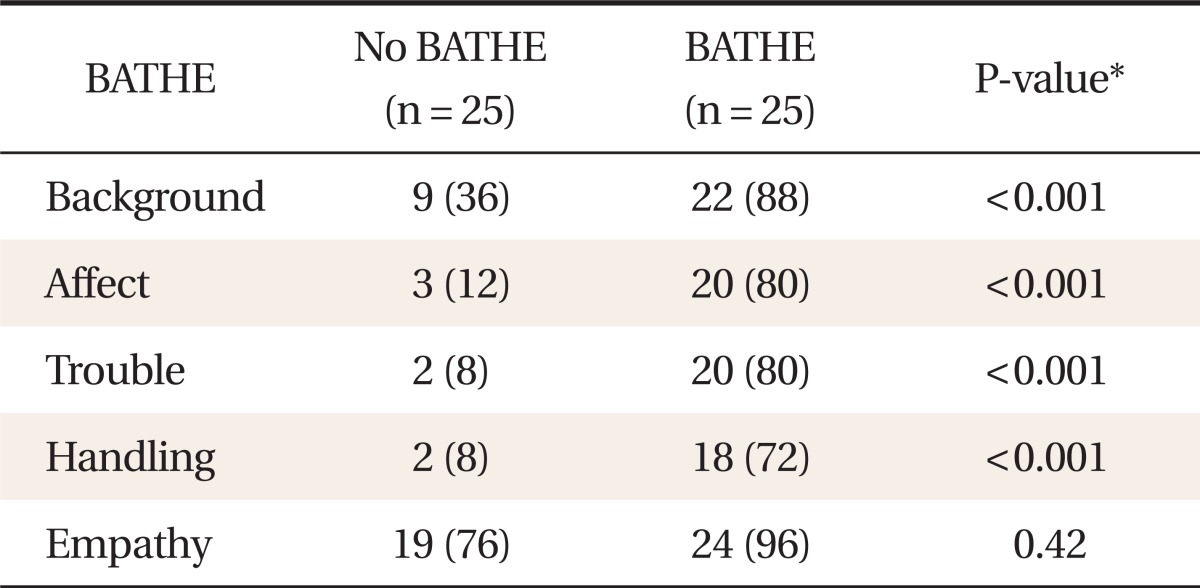
Application of the background, affect, trouble, handling, and empathy (BATHE) components.
3. The Association between the Application of BATHE and Patient Satisfaction
On 7 out of 10 items on the patient satisfaction questionnaire, the BATHE group was found to experience higher level of satisfaction than the control group in a statistically significant manner (P < 0.05). Likewise, on the 10th item alone that rates satisfaction with the overall interview process, the BATHE group was more ready to approve than the control group in a statistically significant manner (P < 0.05) (Table 5); the average score of the BATHE group was 4.7 (± 0.5) while that of the control group was 4.0 (± 0.9). In terms of the total score with the higher score meaning greater satisfaction, the BATHE group scored higher than the control group in a statistically significant manner with the BATHE group scoring 45.8 (± 4.4) on average (Table 5).
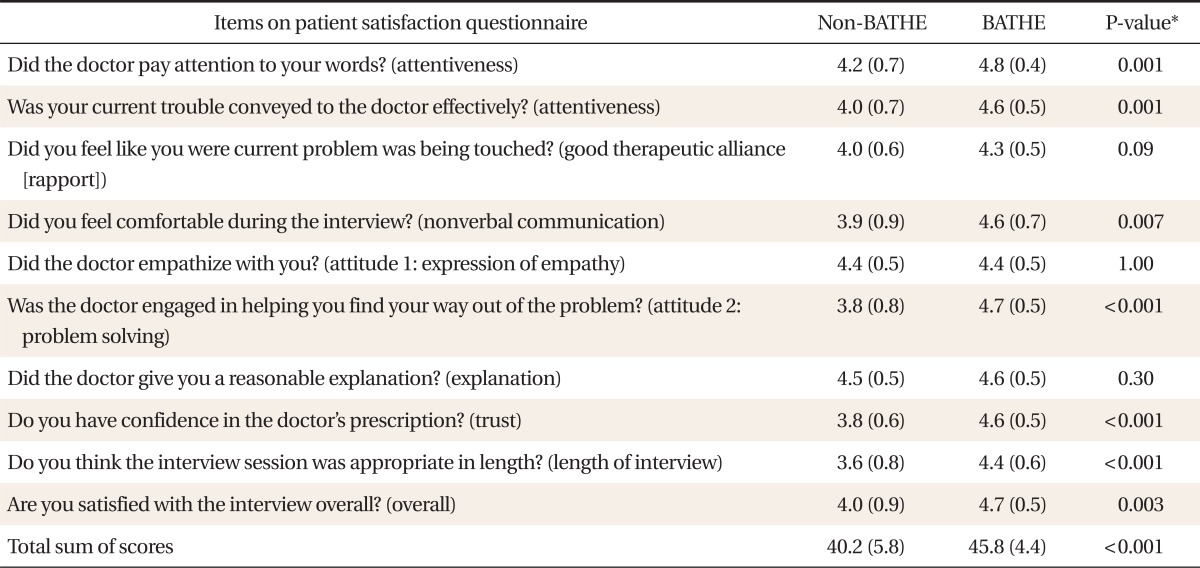
Association between background, affect, trouble, handling, and empathy (BATHE) application and patient satisfaction.
4. The Association between the Application of BATHE and Patient Satisfaction for Each Doctor
For each doctor, on the 10th item of the questionnaire that rates overall satisfaction with the interview process, the BATHE group reported higher satisfaction than the control group in a statistically significant manner (P < 0.05) (Table 6). Likewise, comparing the total score, for each doctor, the BATHE group expressed greater satisfaction than the control group in a statistically significant manner (P < 0.05) (Table 6).
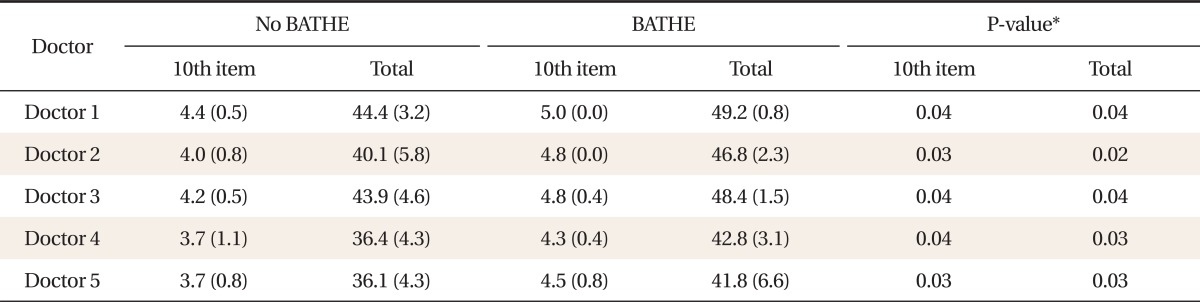
Association between background, affect, trouble, handling, and empathy (BATHE) application and patient satisfaction for each physician.
DISCUSSION
The purpose of this study was to examine whether applying BATHE indeed produces difference in patient satisfaction. Whether the questions asked were appropriate for the interview protocol was evaluated by the researcher through reviewing the video clips taped during the interviews. This study informs us that applying the BATHE interview protocol in outpatient settings is indeed more effective than the usual approach of mere empathy at heightening patient satisfaction.
The items on the patient satisfaction questionnaire represented factors considered essential in patient-oriented interview technique: attentiveness, expression of empathy, nonverbal communication, explanation, good therapeutic alliance (rapport), and length of interview.7) On the two items on attentiveness, the group interviewed using BATHE scored higher, reflecting greater patient satisfaction. The BATHE interview approach, by providing the patient the opportunity to tell his story in order, presumably leads him to feel closely attended to by his interviewer.
However, with respect to the subjective feeling of his problem being touched, the two groups did not differ significantly. There appears to be no difference in patient satisfaction in terms of therapeutic effect between the BATHE and the non-BATHE group.
On the nonverbal communication component, the subjects interviewed using BATHE answered they felt more comfortable during the interview than the control group. The interviewer's attitude was rated by two items, empathy and problem solving. In terms of whether the patient recognized empathy in the interviewer, there was no statistically significant difference between the two groups. However, in terms of whether the patient felt sure of his interviewer's ability in solving his problem, the BATHE group felt more sure than the control group in a statistically significantly manner (P < 0.001). With respect to empathy, there existed no significant difference between the two groups, probably because empathy was common to both the BATHE protocol and the non-BATHE approach.
With regards to whether the patient received reasonable explanation, there was no significant difference between the two groups. On the last two items in the questionnaire, namely trust and length of interview, the BATHE group was more satisfied than the control group in a statistically significantly manner (P < 0.001). This was contrary to our expectations. Even though applying BATHE tends to prolong the interview process, the BATHE group actually reported higher level of satisfaction in terms of interview length (P < 0.001). Regardless of the interviewer, the BATHE group reported higher patient satisfaction than the control group in a statistically significant manner (P < 0.05) which gives us grounds to conclude that BATHE is an interview protocol effective application of which is not user-dependent.
A limitation of this study stems from the inability to extrapolate the findings of this study to the general population owing to the small sample size (five doctors and fifty patients). One can expect validity and reliability to improve, if in further studies, a larger number of family medicine doctors and patients living in a wide range of areas participate. Another limitation of this study is the fact that in selecting subjects for the study, the patient's chief complaint or whether the patient was prescribed medication was not taken into account. Further work is needed to examine whether the patient's chief complaint or whether the patient was prescribed medication affects the effectiveness of BATHE in producing patient satisfaction.
Notes
No potential conflict of interest relevant to this article was reported.