Educational Disparities in Distribution of Cardiovascular Risk Factors and Quality of Care in Korean Adults: Korean National Health and Nutrition Survey IV
Article information
Abstract
Background
The purpose of this study was to investigate how educational status influences cardiovascular risk factors and care of diabetes mellitus and hypertension.
Methods
From Korean National Health and Nutrition Survey IV, we obtained survey results of 6,835 men and 9,067 women more than 30 years old. We performed multivariate logistic regression to compare cardiovascular risk factors and care of hypertension and diabetes respective to educational status.
Results
There were disparities in cardiovascular risk factors by educational status. In men, impaired fasting glucose, high triglyceride, and smoking were less frequently found in the highest educated group than in the middle educated group. In women, the prevalence of abdominal obesity, impaired fasting glucose, high blood pressure, high triglyceride, and metabolic syndrome among the highest educated group were significantly lower. The proportion of those with proper physical activity in the highest educated group was found to be less than that of the middle educated group, regardless of gender. For care of diabetes mellitus and hypertension, disease recognition and treatment were lower among the lowest educated group in men, while these disparities were not shown in women. Instead, the lowest educated group in diabetic women received screening exams for eye and kidney complications less than the middle education group. In both genders, the high education group had a higher chance of receiving education about diabetes mellitus.
Conclusion
There were educational disparities in cardiovascular risk factors and care of hypertension and diabetes mellitus. The disparities were found to be different by gender.
INTRODUCTION
Cardiovascular diseases have been well studied, and their risk factors have been well established. In previous studies, unlike unchangeable risk factors such as family history, many risk factors including abdominal obesity, blood pressure, glucose level, lipid profile, and smoking have been demonstrated to be preventable by lifestyle modification.1-5) However, cardiovascular diseases are still the major cause of death in Korea6) and continue to be a formidable burden on public health. In addition, hypertension and diabetes mellitus may be prevented from advancing to a fatal disease if properly managed.
Educational status has been known to influence the prevalence and prognosis of several diseases7-10) and some previous studies suggests that there is association between educational status and cardiovascular risk factors.11,12) However it has not been clear how educational status affects the management of risk factors. In our study, we assessed the relationship between educational status and cardiovascular disease. Moreover, we also compared quality of care of hypertension and diabetes mellitus to provide effective health services to vulnerable groups.
METHODS
1. Design and Study Population
The Korean National Health and Nutrition Survey (KNHANES) IV is a national health survey in Korea that involves population-based random sampling of 31,705 individuals in 13,800 households across 600 national districts. A stratified multistage probability sampling design (complex sampling design) was applied to the South Korean population. The survey was performed by a rolling sampling survey in 2007, 2008, and 2009. Three samples are representative of the Korean population, homogenous and independent of each other. We performed our analysis with the data collected over three years.
To report educational disparities in cardiovascular risk factors and quality of care of hypertension and diabetes mellitus, we selected proper subjects from the health examination survey for analysis. We started with cross-sectional data from 24,871 participants who had completed the health examination survey. The age was restricted to 30 and over, in order to minimize the misclassification of education status in young participants. Six thousand eight hundred and thirty-five men and 9,067 women attended the health examination and they were included to our study as first subjects. The second subjects are limited to diabetic participants to show the quality of diabetic care. Overall, 742 men and 794 women were enrolled as second subjects. Similarly, hypertensive participants were enrolled as third subjects, with a total of 2,323 men and 2,646 women. Figure 1 shows the model used to select our study population. Finally, with regard to education duration during entire lifetime, we divided subjects into groups of six years and under, seven to twelve years, and over 12 years.
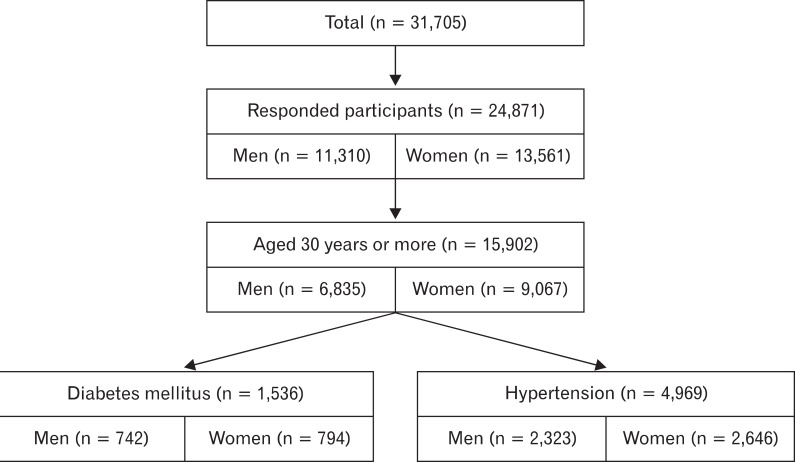
Study population.
2. Outcome Variables
Table 1 shows the definition or criteria of outcome variables in our study.
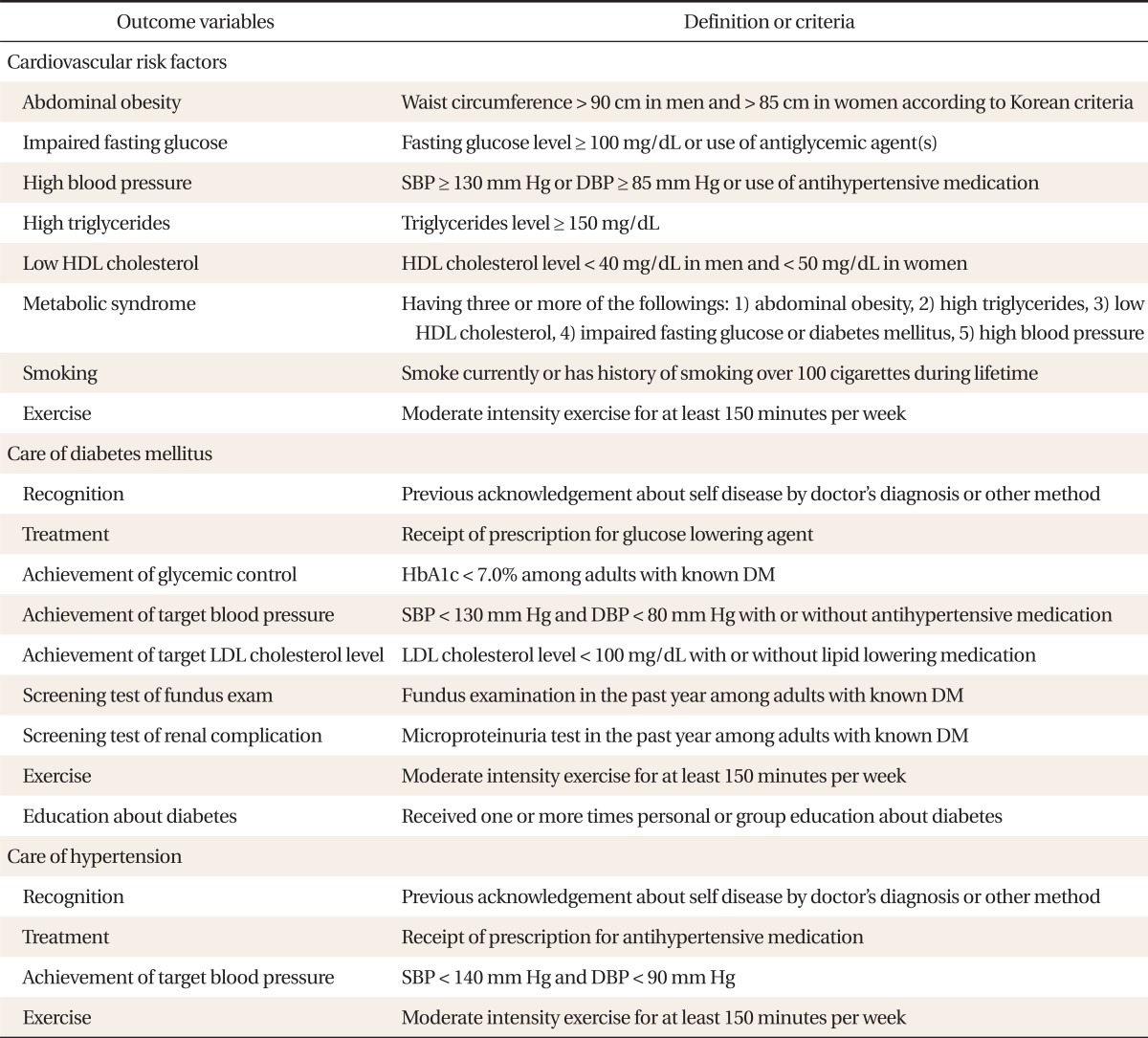
Definition or criteria of outcome variables in this study
1) Cardiovascular risk factors
From KNHANES IV, we obtained data on cardiovascular risk factors. We included age, sex, smoking history, and physical activity. We also included waist circumference, blood pressure, serum glucose, and lipid profile as components of metabolic syndrome,13) all well known risk factors of cardiovascular disease. We did not include family history, an unchangeable risk factor.
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times. We used the mean value of the 2nd and 3rd measurement. High blood pressure was defined as an SBP ≥ 130 mm Hg or a DBP ≥ 85 mm Hg according to the metabolic syndrome criteria.13) Those currently being prescribed with antihypertensive agents were categorized as the high blood pressure group, regardless of their blood pressure. Impaired fasting glucose was defined as a serum glucose level of 100 mg/dL or more, after 8 hours of fasting. Participants already under diabetic treatment were categorized together regardless of their glucose level.13)
From blood pressure, glucose level, waist circumference, and lipid profile, we defined metabolic syndrome.13) Abdominal obesity was defined as waist circumference > 90 cm for men and > 85 cm for women, in reference to the Korean cutoff value.14)
Proper physical activity was defined as subjects undergoing moderate intensity exercise or walking for at least 30 minutes per day and 5 times per week from self-reported questionnaires. Vigorous intensity exercise for at least 20 minutes per day and 3 times per week was also classified as proper physical activity.15) Current smoking was regarded as a risk factor if subjects smoked more than 100 cigarettes throughout their lifetime.
2) Care of diabetes mellitus and hypertension
To assess the quality of health care, we performed analyses in the diabetic and hypertensive subpopulations. In diabetic patients, we assessed recognition of disease, receipt of treatment and education about disease, disease control, management of complication, and proper exercise according to the strong recommendation of American Diabetes Association Guideline 2011.16) In hypertensive patients, we assessed recognition of disease, receipt of treatment, achievement of target blood pressure, and proper exercise.17)
3. Adjustment Variables
All data were separately analyzed by sex. We adjusted for age, the quartile of house income divided by the square-root of number of family members, residence (urban or rural), and personal health insurance. We also adjusted for thought of self-health status (categorized as good, ordinary, or bad) when analyzing quality of care.
4. Statistical Analysis
All data were analyzed using Stata ver. 12.1 (Stata Co., College Station, TX, USA). The age was analyzed using one-way analysis of variance. Socioeconomic status was compared by educational status by chi-square test. To assess cardiovascular risk factors, we used weighted-survey multivariate logistic regression (Stata command; svy: logistic) in order to reflect the characteristics of complex sampling design. However, the sample sizes of diabetes mellitus patients and hypertension patients, the highly selective populations, were too small to calculate standard error by stratified analysis. Therefore, we used conventional multivariate logistic regression without stratification and sampling weight for analysis of care of diabetes mellitus and hypertension. The reference group for logistic regression was selected as the 7 to 12 year education group, which included the majority of the population, to prevent great disparity between the lowest and highest educated group. We also analyzed the linear trend to assess the dose-response relationship.
RESULTS
1. Socioeconomic Status
As shown in Table 2, in both genders, educational status was significantly associated with age, house income, residence, and personal health insurance. The highly educated group consisted of younger and wealthier participants. Moreover, this group is more likely to reside in urban areas and take up personal health insurance.
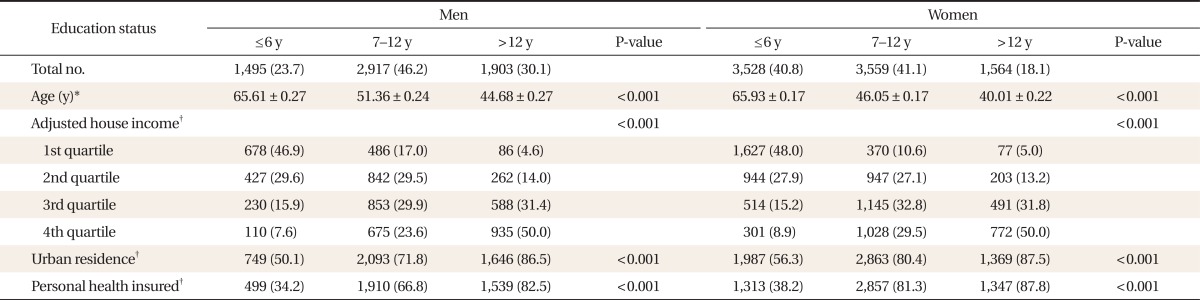
Distribution of socioeconomic status by education and sex
2. Cardiovascular Risk Factors
As shown in Table 3, more educated men smoked less (P for trend < 0.01) and exercised less (P for trend < 0.01). In men, impaired fasting glucose (odds ratio [OR], 0.81; 95% confidence interval [CI], 0.69 to 0.95) and high triglyceride (OR, 0.85; 95% CI, 0.73 to 0.99) were less prevalent in the highest educated groups compared to the reference. In women, education was associated with lower prevalence of all risk factors in a significant linear trend (P for trend < 0.01). It was also associated linearly with less physical activity, a protective risk factor (P for trend = 0.04). Additionally, the prevalence of all risk factors except low high density lipoprotein cholesterol was shown to be significantly lower in the highest educated groups compared to the reference.
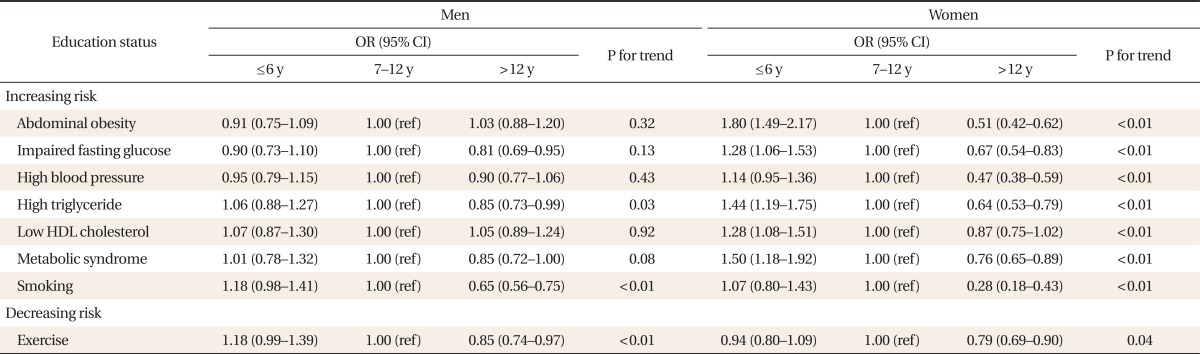
Educational disparity of cardiovascular risk factors by sex
3. Care of Diabetes Mellitus
Table 4 shows the care of diabetes mellitus and hypertension by educational status. Education is associated with recognition of diabetes in men (P for trend = 0.04), while the effect is not apparent in women (P for trend = 0.72). Treatment of diabetes was low in the lowest educated group of men (OR, 0.62; 95% CI, 0.41 to 0.92). However, the highest educated group was associated with a lower chance of receiving treatment in women, although the statistical significance was insufficient (OR, 0.44; 95% CI, 0.19 to 1.03). Achievement of glycemic control was significantly higher in the highest educated group of women (OR, 3.16; 95% CI, 1.30 to 7.68). Achievement of target blood pressure and low density lipoprotein cholesterol level did not show significant differences. More educated groups had a greater tendency to receive fundus examination in men (P for trend < 0.01), whereas the lowest educated group of women received fundus examination less than the reference group (OR, 0.60; 95% CI, 0.39 to 0.94). The result of the urine exam was similar to the fundus exam. For physical activity there were no differences in each group, and the lowest educated groups were associated with a lower chance of receiving education about disease, regardless of gender.
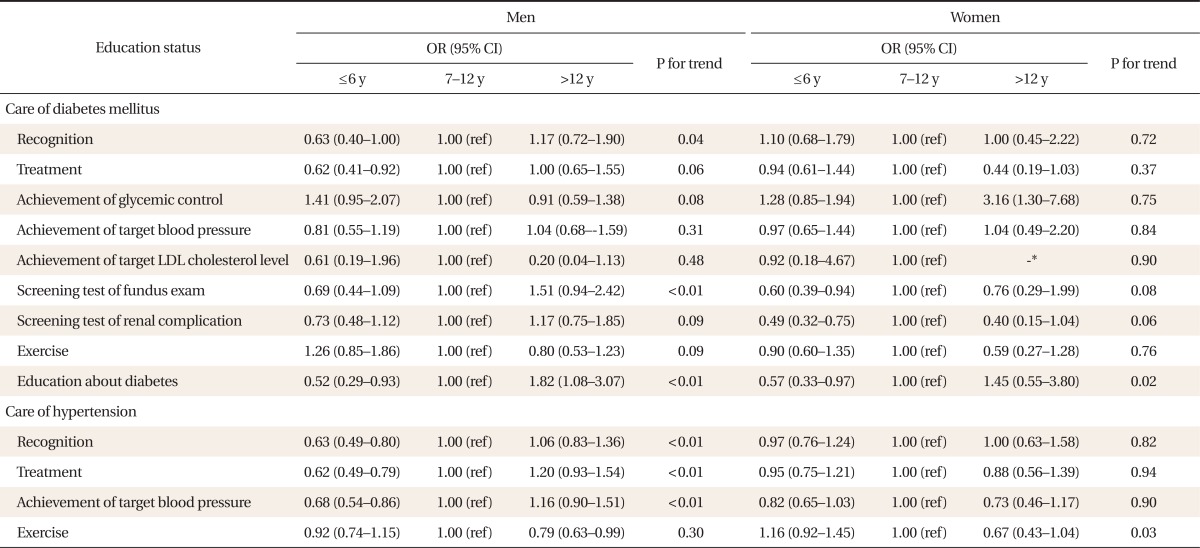
Educational disparity of diabetes mellitus and hypertension care by sex
4. Care of Hypertension
Similar to subjects with diabetes, recognition, treatment and control of hypertension in the lowest educated group were observed to be lower than the reference group in men, while no difference was shown in women. Only the highest educated group in men had significantly less proper physical activity than the reference (OR, 0.79; 95% CI, 0.63 to 0.99).
DISCUSSION
In our study, low educational status of women was associated with a high risk of cardiovascular disease in general. This effect was attenuated in men, but the highest educated group of men still had less risk factors compared to the reference group, specifically, impaired fasting glucose, high triglyceride levels, and smoking, which is consistent with previous studies.11,18) However, some points need to be discussed in our study.
Firstly, educational status has a different effect on cardiovascular risk factors among men and women. We may suspect employment status as the underlying factor creating this sexual difference, because employment also is considered an important factor influencing cardiovascular risk factors.19) According to Korean statistics,20) educational status influences employment more in men than in women. Unfortunately, the results were not changed although adjusting employment status. From a different viewpoint, we used the same cutoff line to classify the educational status in men and women, even though the median year of education was higher in men according to our data. Consequently, the highest educated group of women corresponded to a higher degree of selection compared to that of men, which may have possibly inflated the estimates.
Secondly, there was inconsistency with a previous study,21) in that the highest educated group was less physically active than the reference group. Our study was limited as a cross-sectional study. The causal relationship between factors cannot be determined, and reverse causality is always a possibility. For example, the highest educated group may be less motivated to exercise due to lower prevalence of other cardiovascular risk factors. Nevertheless, considering the fact that physical activity is beneficial to various medical conditions,17) it is undeniable that physical activity in the highest educated group is insufficient.
Regarding care of diabetes mellitus, there were some significant disparities by educational status, and these findings were consistent with a previous study.22) We observed some differences in treatment in men and achievement of glycemic control in women. However, a consistent difference was apparent in education related to disease. It is already well known that education takes an important role in diabetic care.23) Although the guidelines recommend that all new patients receive "diabetes self-management education", only fifteen percent of participants answered that they have received diabetic education, and our results suggest that fewer among the lowest educated group receive education about disease. We could assume that the more educated group may have more opportunities to assess microvascular complications through fundus and renal screening. When we adjusted for education about diabetes, although this data was not shown, the association was no longer apparent. It suggests that the major factor to improve care is not educational status, which is an unchangeable factor of the past, but current education about disease.
Concerning exercise, the disparity between groups was minimal compared to the results of cardiovascular risk factors. We can thus assume that the major confounding factor related to exercise may be current disease status, especially diabetes mellitus.
Regarding care of hypertension, more education seemed to lead to better quality of care in men, while this tendency was attenuated in women. In our data, only 5 percent of those who had been previously diagnosed with hypertension reached the target goal of blood pressure without medication. On the contrary, the association between medication use and diabetic control appears to be weak. Our data suggest that the adherence to physician's orders may be more important in hypertension than self-awareness.24,25) Conclusively, education may have the effect of increasing adherence to physician's orders in men, while decreasing adherence in women, even though the effect appeared to be statistically insignificant.
According to a previous study,26) these disparities might be associated with a knowledge gap. Misconception that cardiovascular disease is not preventable was frequently shown in less educated people, and this could impede modification of lifestyle and receipt of proper care. High risk and poor care, interacting viciously among the lowest educated group, may be associated with increased mortality.27) Health care and education about disease provided by educational status are expected to contribute to lower advanced disease and mortality effectively.
Conclusively, we found that there were educational disparities in cardiovascular risk factors and care of hypertension and diabetes mellitus. The disparities were found to be different by gender.
Notes
No potential conflict of interest relevant to this article was reported.