INTRODUCTION
Although the Korean medical culture and environment is different from western health care systems, family physicians are essential in primary care practices in Korea. Well-trained family doctors are necessary to meet the needs of patients and the community. Therefore, all those involved in family medicine education, including medical school professors, preceptors, residency program faculty, and residency program directors play a crucial role in the development of family medicine practitioners. This is especially true because family medicine resident training staffs provide training with regard to not only knowledge or skills related to medical practice, but also diverse topics related to the characteristics and philosophy of family medicine. As such, their roles are more comprehensive than the roles of other specialized medical teachers.
Organizations such as the Society of Teachers of Family Medicine (STFM)1) and the European Academy of Teachers of General Practice2) in Western countries provide official courses for the development of Korean family medicine resident training staffs. Thirty-four years have passed since the first family medicine residency program was introduced in Korea, and in 2011 alone, more than 1,000 family medicine residents were trained by 278 family medicine faculty members at 154 hospitals.3) Regardless, there have been few faculty development programs or specialized courses for family medicine resident training staffs in Korea. Accordingly, for the establishment of faculty development programs in the future, we designed this study to assess the need for faculty development among Korean family medicine resident training staffs.
METHODS
1. Subjects
We surveyed family medicine resident training staff members, including medical school professors and faculty, as well as community-based residency program directors and faculty. The institutional review board of Chung-Ang University Hospital approved the study. We obtained online informed consent for participation.
2. Questionnaire
The survey used in this study is a modified version of a previously unpublished questionnaire used by the Korean Academy of Family Medicine (KAFM)3) together with faculty competency assessment checklists developed by Harris et al.4) The survey included questions regarding the demographics of the respondents, satisfaction with their current family medicine residency programs, the difficulties involved in resident training, and the perceived need for faculty development programs. Respondents rated items on a five-point Likert scale (with levels of difficulty ranging from 1 = very easy to 5 = very difficult). Staff member satisfaction was measured on a 0-10 visual analogue scale.
3. Data Collection
We obtained the e-mail addresses of all 278 family medicine resident training staff members through the KAFM to be used exclusively for this study. The survey was conducted using OZsurvey (http://www.ozsurvey.co.kr), an online survey tool, between April and June of 2010. The questionnaires were sent to family medicine resident training staff members by e-mail a total of three times at intervals of three weeks for the duration of the survey period.
4. Statistical Analyses
For analyses, we divided subjects into several groups based on type of hospital (tertiary medical school teaching hospital, secondary medical school teaching hospital, and non-medical school teaching hospital), role of hospital (main or satellite), and the number of staff members (1 vs. Ōēź2). The general characteristics were presented as number (%). For comparing aspects of satisfaction and difficulty according to the general characteristics of the staff members, Pearson's correlation, Student t-test, and/or analysis of variance tests were conducted. Statistical analyses were performed using the SAS ver. 9.1 (SAS Institute Inc., Cary, NC, USA).
RESULTS
1. General Characteristics
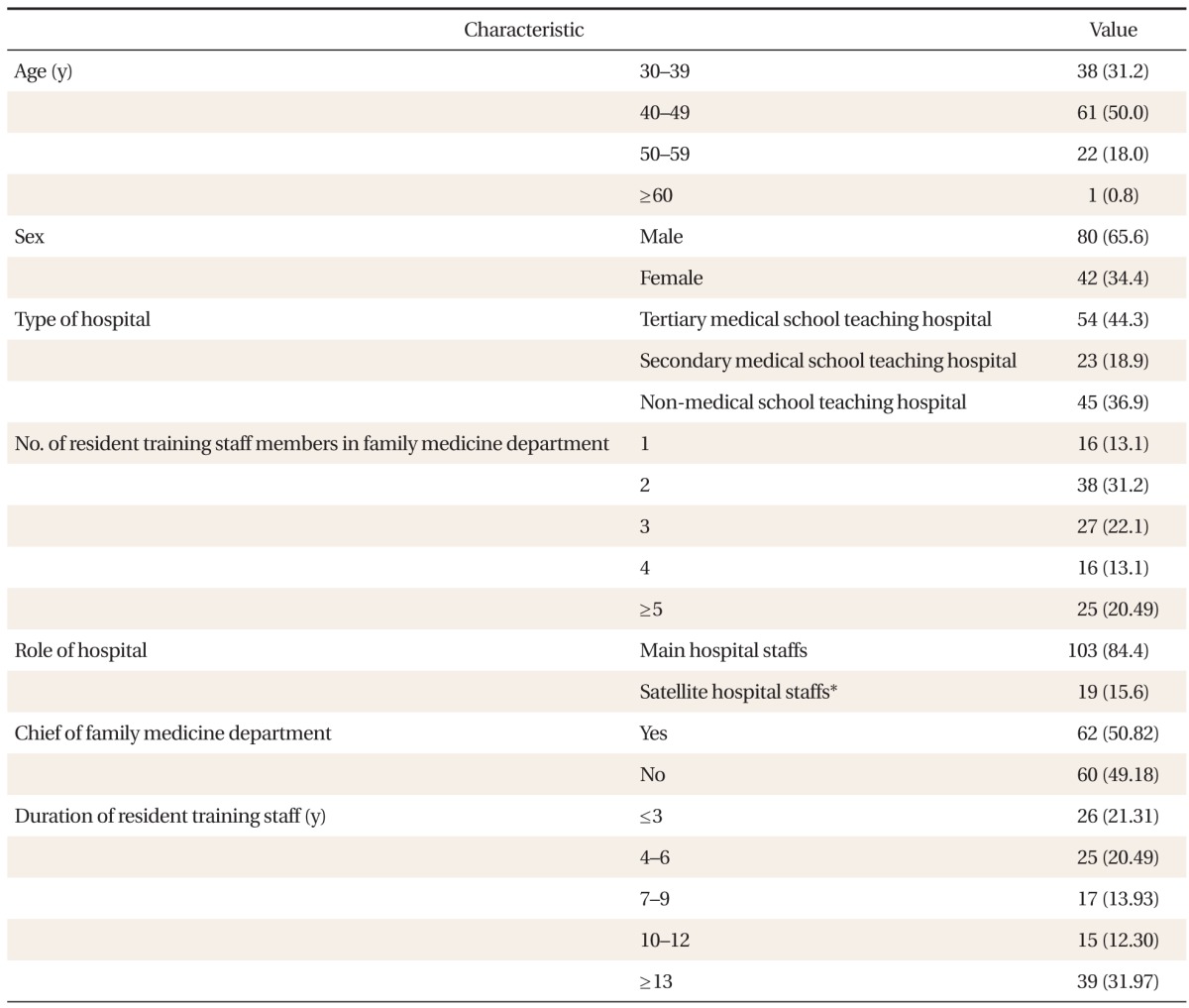
Of the 278 resident training staff members in various family medicine departments, 122 staff members (43.9%) completed the survey. The characteristics of participants are shown in Table 1. The majority of staff members were 40 to 49 years of age (50.0%). Approximately two-thirds of all respondents were male (65.6%). The mean number of resident trainers was 3.84 (┬▒ 2.49) per staff. The mean duration of being a family medicine teacher was 9.53 ┬▒ 6.64 years.
2. Satisfaction with Residency Programs among Family Medicine Staffs
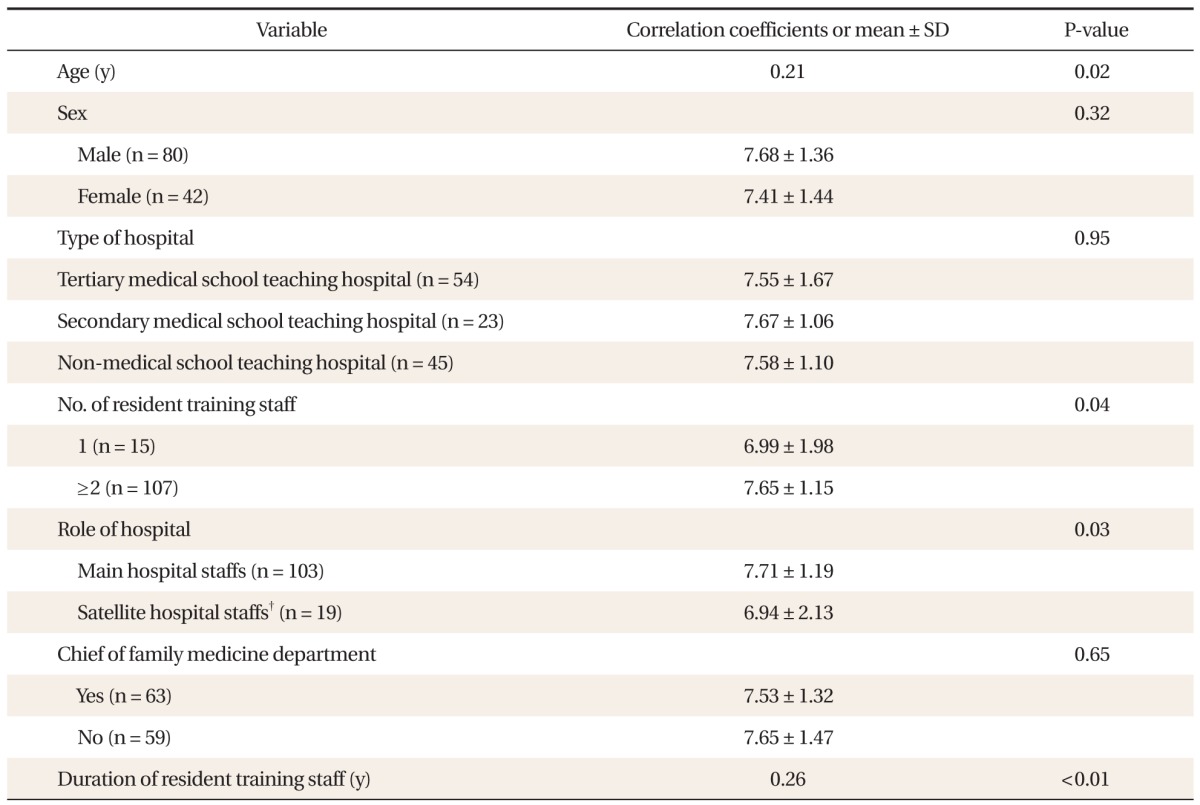
The mean score of satisfaction with current family medicine residency programs was 7.59 (┬▒ 1.39) out of 10. Satisfaction scores toward current residency programs increased with the age of staff members (P = 0.02) and duration of staff members (P < 0.01). In cases where the family medicine department staff consisted of only one member, the satisfaction of the training staff was lower (P = 0.04). The satisfaction of satellite hospital staffs was lower than the satisfaction of main hospital staffs (P = 0.03) (Table 2).
3. Reported Difficulties of Resident Training among Family Medicine Staffs
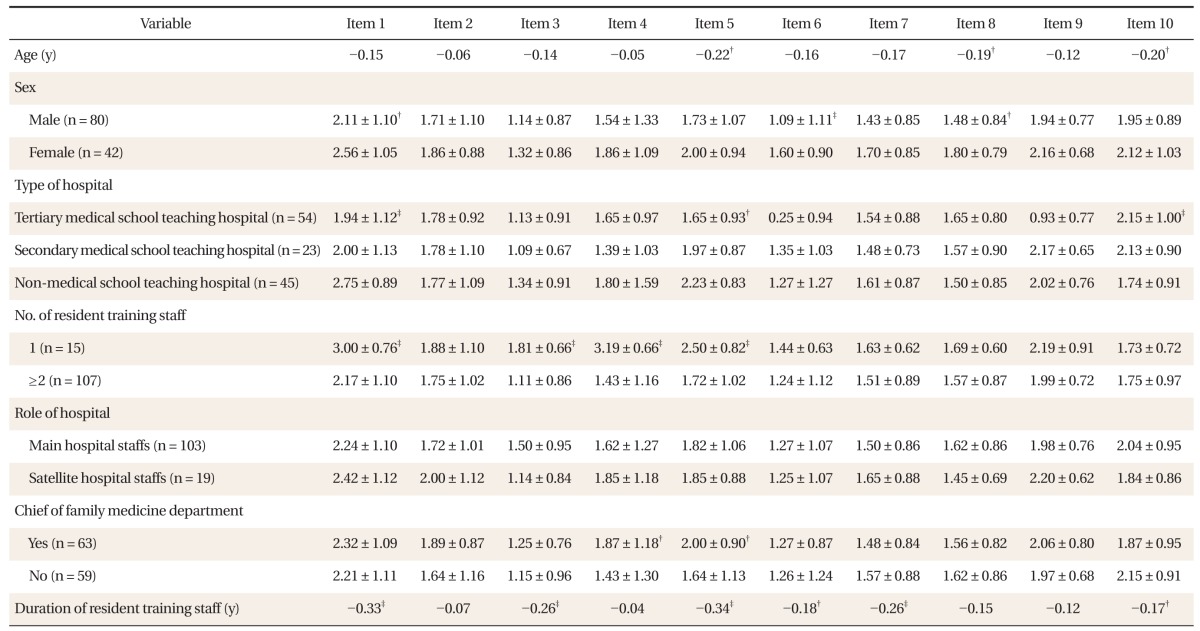
Respondents reported difficulties with resident training in the following order: administration (2.27 ┬▒ 1.10), development of good relationships with their institutions (2.02 ┬▒ 0.74), teaching clinical skills (2.01 ┬▒ 1.03), having the role of research director (1.82 ┬▒ 1.03), communication with residents (1.77 ┬▒ 0.94), design of training in specialized departments (1.65 ┬▒ 1.26), preceptors in outpatient clinics (1.59 ┬▒ 0.84), lack of instructional resources (1.52 ┬▒ 0.86), insufficient number of family medicine instructors (1.27 ┬▒ 1.07), and the organization of conferences (1.20 ┬▒ 0.86).
Perceived difficulties related to resident training decreased with the age and duration of staff members regarding several items in the survey (Table 3). Female staff members found it more difficult to act as administrators and preceptors in outpatient clinics than male staff members. Female staff members also felt that the number of resident trainers per staff was insufficient. Perceived levels of difficulty with administration, the role of research director, and the teaching of clinical skills were significantly different among the 3 types of hospitals. Administration was thought to be more difficult among staffs of non-medical school teaching hospitals than among the staffs of the other 2 groups (P < 0.01). The role of research director was thought to be more difficult in secondary or non-medical school teaching hospital staffs than in tertiary medical school teaching hospital staffs (P = 0.03). In comparison to non-medical school teaching hospital staffs, however, the family medicine staffs of secondary or tertiary medical school teaching hospitals reported more difficulty in the teaching of clinical skills (P = 0.04). Conference organization, design of training in specialized departments, and having the role of research director were difficult aspects among the solo staffs surveyed (P < 0.01). Among those designated as chiefs of family medicine departments, the design of training in specialized departments (P = 0.04) and the role of research director (P = 0.04) were more difficult than among nonchief staff members (Table 3). Also, most respondents (91.9%) cited a need for faculty development programs.
DISCUSSION
We determined that family medicine resident training staffs are not fully satisfied with their current residency programs and would benefit from programs for faculty development. Interestingly, there were considerable differences in the reported difficulties of resident training, and in the need for faculty development, according to differing characteristics of each staff.
It is more difficult to play the role of research director in non-medical school teaching hospital staffs than in medical school teaching hospital staffs. Previous research showed that staffs of non-medical school teaching hospitals, or the staff of a teaching hospital for only family medicine, contributed little to the research of academic advisers.5) These results can be attributed to several factors. Non-medical school teaching hospital staffs, especially the staff of a teaching hospital for only family medicine, have little experience with research or with human resources and the physical infrastructure for basic or clinical studies. Based on data from the KAFM, the number of teaching hospitals that focus only on family medicine was 39 (28.5%) in 2012. Accordingly, the KAFM needs to provide programs on research methods and article preparation for residents in those hospitals.
Teaching clinical skills is reportedly the most difficult item among medical school teaching hospital staffs. Non-medical school teaching hospital staffs, however, reported that teaching clinical skills is less difficult in comparison to reports from tertiary or secondary medical school teaching hospital staffs. It was previously reported that the teaching of a gastroscopy examination as a notable clinical skill is not easy for most large-scale hospitals, with the exception of well-connected family medicine departments with health examination centers.6) The acquisition of clinical skills is essential for primary care physicians. Therefore, at the academic level, it is necessary to consider the introduction of suitable and independent teaching hospital systems in which residents can obtain firsthand experience with various clinical skills under expert supervision.
Furthermore, this survey shows that there are many differences in the characteristics and needs of solo staff members and staffs with two or more members in family medicine departments in Korea. Comparing a staff of only one member in a family medicine department to staffs with two or more members, the age of the staff was younger (41.13 ┬▒ 4.38 vs. 48.2 ┬▒ 6.16 years, P = 0.01), and the number of trainers per staff was higher (6.00 ┬▒ 3.39 vs. 3.52 ┬▒ 2.17, P = 0.01). Also, the duration of staff was shorter among solo staff members (6.69 ┬▒ 4.47 years) than among staffs with two or more members in family medicine departments (9.95 ┬▒ 6.82 years, P = 0.02). Most solo staff members (81.25%) practiced in non-medical school teaching hospitals. The remaining solo staff members practiced in secondary medical school teaching hospitals. The solo staff members reported great difficulty in administration, conference organization, design of training in specialized departments, and the role of research director. Therefore, in order to support teaching in environments with a single staff member, the provision of diverse training resources and faculty development programs through the KAFM is essential. Recently, online videoconferencing systems have been reported useful for medical education.7,8) Implementation of multichannel videoconferencing by an extensive network among family medicine departments may reduce the difficulties of conference organization for staffs.
The Faculty Futures Initiative has reported that the expected competencies and roles of family medicine faculty include administrators, educators, researchers, and clinicians.9) Although there are distinct roles and responsibilities in every hospital, all family medicine teachers are expected to have core competency skills such as leadership, administration, teaching, research, medical informatics, and multiculturalism.4) The results of our survey indicate that programs or courses for the development of family medicine teachers must be designed and implemented in Korea. Different levels of faculty development are particularly necessary in different situations (e.g., for fellows, early resident training staffs, chief, tertiary or secondary hospital resident training staffs, and medical school or non-medical school teaching hospital resident training staffs within family departments). Faculty development programs such as the National Institute for Program Director Development Fellowship10) or the New Faculty Development Series Workshop of STFM1) have been undertaken in the US. In recent years in Korea, workshops for resident training staffs have been conducted at the annual congress. Furthermore, it will not be long before certificate systems for resident training staffs are introduced. Therefore, it is necessary to establish faculty development programs that include high-quality contents.
There are several limitations to this study. First, the response rate was only 43.9%. However, this response rate is not too low in comparison to the response rate of resident training staffs in other studies.11) Second, this study's questionnaire may not completely reflect the needs of resident training staffs because we did not examine a more robust picture with the use of a pilot survey. Nevertheless, it is significant that this is the first study to assess the need for faculty development among resident training staffs in Korean family medicine departments.
In conclusion, we find that resident training staffs in Korean family medicine departments are not satisfied with their current residency programs, and that they need faculty development programs for the improvement of resident training. For the strengthening of expected core competencies among resident training staffs, customized faculty development programs and courses should be designed and implemented in Korea.