Validity of Alcohol Use Disorder Identification Test-Korean Revised Version for Screening Alcohol Use Disorder according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition Criteria
Article information
Abstract
Background
The Alcohol Use Disorder Identification Test (AUDIT) has been widely used to identify alcohol use disorder (AUD). This study evaluated the validity of the AUDIT-Korean revised version (AUDIT-KR) for screening AUD according to Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria.
Methods
This research was conducted with 443 subjects who visited the Chungnam National University Hospital for a comprehensive medical examination. All subjects completed the demographic questionnaire and AUDIT-KR without assistance. Subjects were divided into two groups according to DSM-5 criteria: an AUD group, which included patients that fit the criteria for AUD (120 males and 21 females), and a non-AUD group, which included 146 males and 156 females that did not meet AUD criteria. The appropriate cut-off values, sensitivity, specificity, and positive and negative predictive values of the AUDIT-KR were evaluated.
Results
The mean±standard deviation AUDIT-KR scores were 10.32±7.48 points in males and 3.23±4.42 points in females. The area under the receiver operating characteristic curve (95% confidence interval, CI) of the AUDIT-KR for identifying AUD was 0.884 (0.840–0.920) in males and 0.962 (0.923–0.985) in females. The optimal cut-off value of the AUDIT-KR was 10 points for males (sensitivity, 81.90%; specificity, 81.33%; positive predictive value, 77.2%; negative predictive value, 85.3%) and 5 points for females (sensitivity, 100.00%; specificity, 88.54%; positive predictive value, 52.6%; negative predictive value, 100.0%).
Conclusion
The AUDIT-KR has high reliability and validity for identifying AUD according to DSM-5 criteria.
INTRODUCTION
Many questionnaires have been designed for the early detection of alcohol use disorder (AUD), including the Alcohol Use Disorder Identification Test (AUDIT), developed by the World Health Organization. The AUDIT is composed of 10 questions addressing the quantity and frequency of alcohol consumption and is particularly useful for screening for heavy drinking and binge drinking.1) In Korea, heavy drinking and binges are common forms of alcohol abuse; thus, several studies have been conducted to confirm the validity of the Korean-language AUDIT for screening for AUD in Korea. In 1999, Kim et al.2) confirmed that the AUDIT is a useful screening tool for AUD in Korea. They suggested cut-off values of 12 or more for problem drinking, 15 or more for AUD, and 26 or more for alcohol dependence.
However, because questions 2 and 3 defined one standard drink as 14 g of pure alcohol, AUDIT was difficult to apply in Korea. In Korea, a variety of alcoholic beverages are consumed, and the serving size changes depending on the type of alcohol. In 2014, Kim et al.3) developed the AUDIT-Korean revised version (AUDIT-KR), which overcame these problems. According to this study, the appropriate cut-off value for AUD was 10 for males and 8 for females.
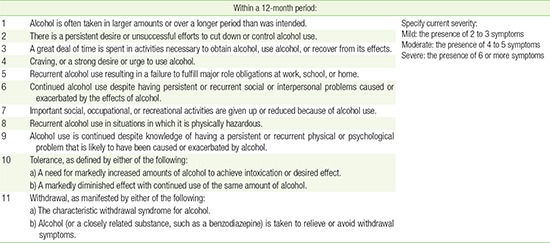
The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) was created by the American Psychiatric Association4) and revised in 2013 (Appendix 1). In the DSM, fourth edition (DSM-IV), AUD was divided into alcohol abuse and alcohol dependence. However, in the DSM-5, these categories were integrated into AUD, and the severity of AUD was classified into three levels: mild, moderate, and severe.5) Additionally, the DSM-IV criterion regarding legal problems was eliminated, and a criterion about craving alcohol was added. The DSM-5 definition of AUD is composed of 11 criteria. Satisfying two or three criteria within the past 12 months is defined as mild AUD, satisfying four or five as moderate AUD, and satisfying more than six as severe AUD.
The objective of this study was to verify the validity of the AUDIT-KR for screening for AUD according the DSM-5 criteria and to determine appropriate cut-off values.
METHODS
1. Subjects
This study was conducted among patients who visited the health promotion center of Chungnam National University Hospital for a comprehensive medical examination from December 2014 to May 2015. Initial interviews included 500 participants who agreed to complete a demographic questionnaire and the AUDIT-KR. Fifty-seven respondents who did not fully complete the questionnaires were excluded. The AUD group consisted of 141 subjects (male, 120; female, 21), while the non-AUD group consisted of 302 subjects (male, 146; female, 156), with groups being formed based on the results of the interview and DSM-5 criteria. This study was approved by the institutional review board of Chungnam National University Hospital. The study protocol followed the Declaration of Helsinki and included written consent by the participants.
2. Diagnosis and Data Collection
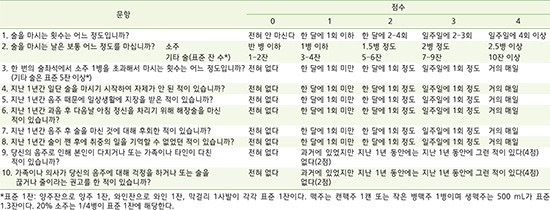
Subjects completed the demographic questionnaire and AUDIT-KR without assistance. The version of the AUDIT-KR created by Kim et al.3) in 2014 was used (Appendix 2). Demographic data, such as age, smoking history, educational level, marital status, employment, and religion, were also collected.
Subjects were interviewed, and classified into AUD or non-AUD groups according to DSM-5 criteria. Subjects who met two or more criteria were diagnosed with AUD and classified into the AUD group. Subjects who met fewer than two criteria were classified into the non-AUD group.
3. Data Analysis
A chi-square test was used to compare categorical demographic variables (smoking history, educational level, marital status, and employment) between the AUD and non-AUD groups. Between-group comparisons of continuous variables (age and AUDIT-KR score) were performed using the Student t-test. The receiver operating characteristic (ROC) curve and area under the ROC curve (AUROC) of the AUDIT-KR scores were obtained to determine the ability of the AUDIT-KR to identify AUD in male and female subjects. The sensitivity, specificity, positive predictive value, and negative predictive value of each cut-off value were calculated. The most appropriate cut-off value was determined by the highest Youden index, which is the sum of sensitivity and specificity. Data analysis was performed with IBM SPSS ver. 21.0 (IBM Co., Armonk, NY, USA) and MedCalc Statistical Software ver. 15.6 (MedCalc Software, Mariakerke, Belgium). P-values less than 0.05 were considered significant.
RESULTS
1. Demographic Characteristics and Alcohol Use Disorder Identification Test-Korean Revised Version Scores of the Subjects
Of the 443 respondents, 266 were male and 177 were female. The mean age of the male and female differed significantly (51.84±11.14 years and 48.84±10.11 years, respectively; P-value=0.004) (Table 1). There were a significantly higher proportion of current smokers in males than in the females (34.1% vs. 5.3%, P-value <0.001). There were also significant differences between males and females with regard to educational level, employment, and religion. However, there were no significant differences in marital status between males and females. The average AUDIT-KR score was significantly higher in the males than in the females (10.32±7.48 points vs. 3.23±4.42 points, P-value <0.001).
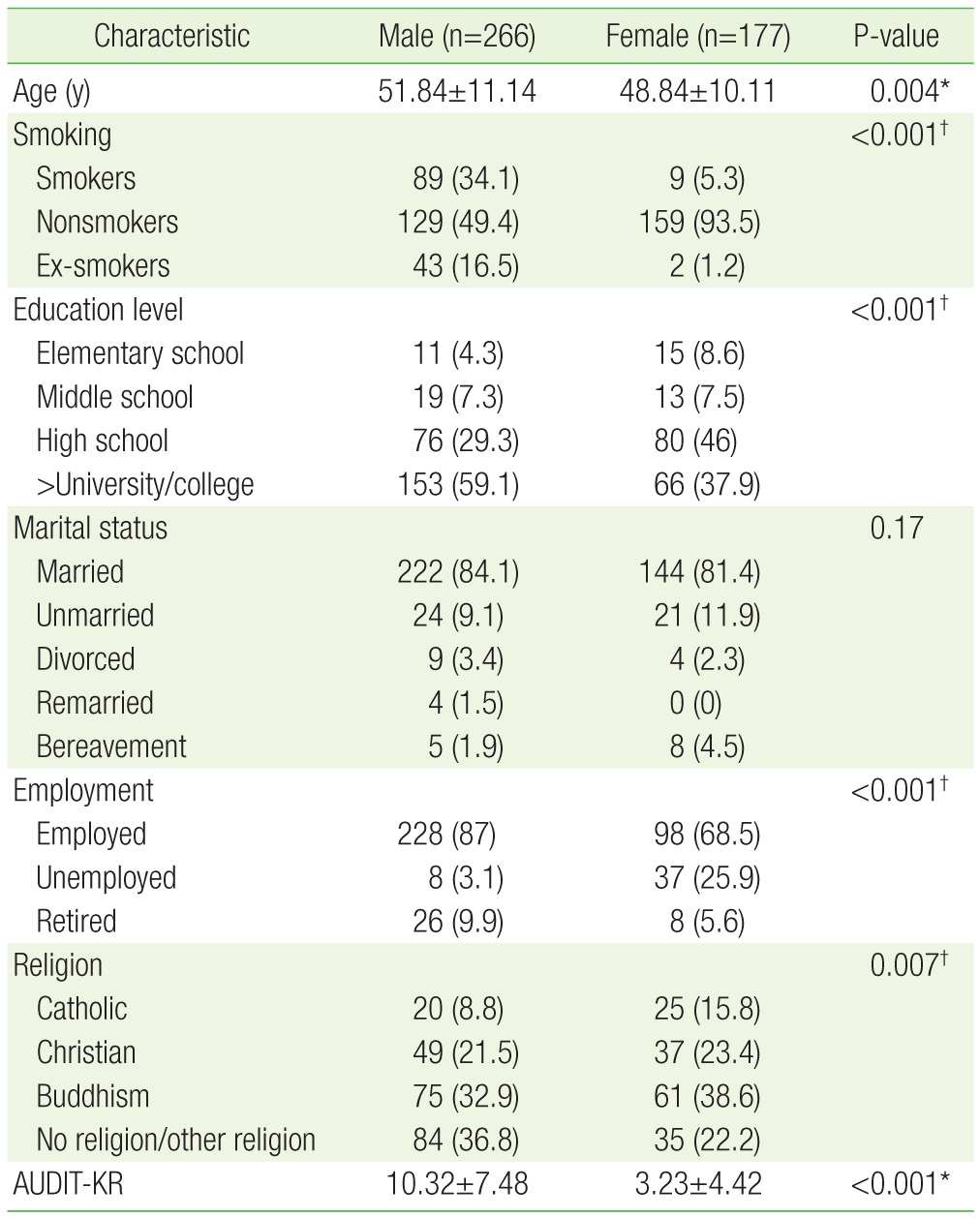
General characteristics and mean AUDIT-KR scores of subjects
2. Validity of the Alcohol Use Disorder Identification Test-Korean Revised Version and Optimal Cut-Off Values for Alcohol Use Disorder Screening
The AUROC (95% confidence interval, CI) of the AUDIT-KR with regard to screening for AUD was 0.884 (0.840−0.920) for male subjects and 0.962 (0.923−0.985) for female subjects (Figure 1). An appropriate cut-off value for AUD screening in males was 10 points. At this value, the Youden index was 0.6323; the sensitivity and specificity of the AUDIT-KR were 81.90% and 81.33%, respectively; and the positive and negative predictive values were 77.2% and 85.3%, respectively. An appropriate cut-off value for AUD screening in females was 5 points. At this value, the Youden index was 0.8854; the sensitivity and specificity of the AUDIT-KR were 100.0% and 88.54%, respectively; and the positive and negative predictive values were 52.6% and 100.0%, respectively (Table 2).
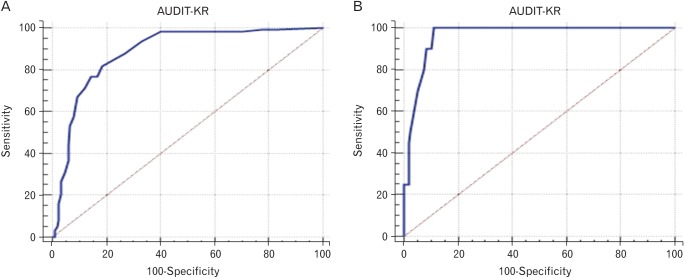
Receiver operating characteristic curves of AUDIT-KR for identifying alcohol use disorders according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition criteria. (A) Male: AUROC (95% CI)=0.884 (0.840–0.920). (B) Female: AUROC (95% CI)=0.962 (0.923–0.985). AUDIT-KR, Alcohol Use Disorders Identification Test-Korean revised version; AUROC, area under the receiver operating characteristic curve; CI, confidence interval.
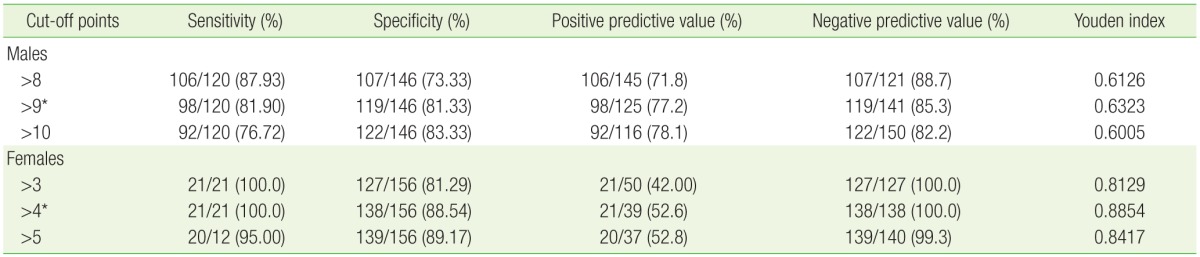
Cut-off points and performance of Alcohol Use Disorder Identification Test-Korean revised version for identifying alcohol use disorder according to Diagnostic and Statistical Manual of Mental Disorders, fifth edition criteria
DISCUSSION
The recently revised DSM-5 integrated the categories of alcohol abuse and alcohol dependence into AUD, and patients fulfilling two or more DSM-5 criteria meet the diagnostic criteria for AUD. The severity of AUD was classified into three levels: fulfillment of two or three criteria defines mild AUD, fulfillment of four or five defines moderate AUD, and fulfillment of six or more defines severe AUD. Because of this change in AUD diagnostic criteria, it is necessary to confirm the validity of existing questionnaires in screening for the presence of AUD in a Korean population. Until now, the AUDIT-KR has been a valuable tool for AUD screening in Korea. This study examined the differences in AUDIT-KR scores between AUD and non-AUD groups and the validity of the AUDIT-KR according to DSM-5 criteria.
In this study, an appropriate cut-off value when using the AUDIT-KR for AUD screening was 10 points for males and 5 points for females. The cut-off values suggested in the present study were higher than those suggested by Kim et al.3) in 2014: 3 points for all at-risk people. Compared with previous studies, the cut-off value for AUD was the same in males (10 points) and lower in females (8 points).3) This discrepancy may have resulted from the changes in the diagnostic criteria for AUD in the DSM-5 compared with the DSM-IV. We used the DSM-5 diagnostic criteria for classifying the AUD and non-AUD groups. There were two major changes in the diagnostic criteria from the DSM-IV to the DSM-5. First, the diagnoses of alcohol abuse and alcohol dependence were integrated into the diagnosis of AUD. Second, the DSM-IV criterion about legal problems was eliminated, and a criterion about alcohol craving was added.46) Because of these changes, the DSM-5 regrouped AUD patients and also potentially changed optimal cut-off values for screening questionnaires.
Some reports have suggested regrouping AUD patients according the new diagnostic criteria. The study conducted by Mewton et al.7) suggested that only 50% of patients diagnosed with AUD under the DSM-IV were diagnosed with this condition under the DSM-5 and that 40% of AUD patients were newly diagnosed according to DSM-5 criteria. Although the degrees of discrepancy differed, other articles also found that some AUD patients were newly diagnosed under DSM-5 criteria.8910111213) Therefore, we hypothesized that AUD patients would be regrouped under the DSM-5, and that the optimal cut-off values would also be redefined. However, because our study did not include the criterion regarding legal problems, a direct comparison between DSM-IV and DSM-5 could not be performed. Further research is needed to examine the diagnostic concordance between DSM-IV and DSM-5 in Korea.
In the present study, the AUROC (95% CI) of the AUDIT-KR in screening for AUD was 0.884 (0.840−0.920) for males and 0.962 (0.923−0.985) for females. An AUROC value of 1 signifies a perfect diagnostic tool; a value lower than 0.5 reflects the inappropriateness of a diagnostic tool. Thus, the closer the AUROC value is to 1, the better it is as a diagnostic tool.14) The AUROC results in our study suggested that the AUDIT-KR was an appropriate diagnostic tool for screening for AUD according to DSM-5 criteria. A previous article from the United Kingdom reported that the AUDIT was useful for AUD screening in both genders, ranging in age from 18 to 35 years according to DSM-5 criteria (males: AUROC, 0.70; 95% CI, 0.60 to 0.78; females: AUROC, 0.73; 95% CI, 0.67 to 0.78).15) The AUROC results in that article were lower than the results found by our study. This discrepancy was most likely due to the ages of subjects. In Korea, Kim et al.3) conducted a study to verify the validity of the AUDIT-KR for AUD screening according to DSM-IV criteria. This study suggested that the AUDIT-KR was useful for AUD screening, with AUROC results of 0.946 (95% CI, 0.918 to 0.975) for male subjects and 0.898 (95% CI, 0.857 to 0.939) for female subjects. Among male subjects, the AUROC in the current study (0.884) was lower than that found by Kim et al.3) and among female subjects, the AUROC in the present study (0.962), was higher than that in the previous one. Thus, the AUDIT-KR was more effective in males under DSM-IV criteria, but it is now more effective in females under DSM-5 criteria.
To our knowledge, this is the first study to confirm the validity of the AUDIT-KR for AUD screening according to DSM-5 criteria. The AUDIT-KR remains an effective tool for AUD screening, especially with regard to the changes made to the AUDIT to reflect the Korean culture of alcohol consumption.
There are several limitations concerning the generalization of the results obtained in the current study. First, because this was a screening accuracy test, we could not identify the prevalence of AUD according to DSM-5 diagnostic criteria. Second, the subjects in the present study were limited to patients from only one hospital, and selection bias might have affected our results. To address this issue, a similar study of the Korean general population is needed. Finally, the number of female subjects in AUD group was small. The AUROC of females could be affected by this limitation and might be artificially elevated when compared to the actual value.
Despite these limitations, it is meaningful that this is the first study to confirm the validity of the AUDIT-KR, as well as suggesting optimal cut-off values according to DSM-5 criteria. Furthermore, the current study suggests cut-off values for each gender, providing an effective tool for AUD screening in clinics.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Appendices
Appendix 1
Alcohol use disorder criteria of the Diagnostic and Statistical Manual of Mental Disorders, fifth edition4)
Appendix 2
Alcohol Use Disorders Identification Test-Korean revised version3)