INTRODUCTION
Depression is a mood disorder with symptoms that include persistently depressive mood, loss of motivation or interest, and feelings of guilt. Severe cases may be accompanied by eating and memory disorders, and may also lead to suicide.1) The data from the 2005ŌĆō2008 National Health and Nutrition Examination Survey conducted in the United States reported that approximately 21.6% of participants showed depressive symptoms,2) whereas the World Health Organization World Mental Health (2004) Surveys reported lifetime prevalences of major depressive disorders of 19.2%, 21.0%, and 17.9% for the United States, France, and the Netherlands, respectively.3) Based on the 2011 Epidemiological Survey of Mental Disorders in Korea from the Ministry of Health and Welfare, 6.7% of participants 18 years and older experienced major depressive disorders at least once in their lifetimes.4) The prevalence of major depressive disorders in Korea is lower than that reported in other countries. This observation is interpreted as a sociocultural difference, in that Far East Asian cultures do not satisfy the diagnostic criteria for major depressive disorders: assessments often reveal no major symptoms because the individuals themselves consider depressive symptoms to be mild conditions.5)
In 1988, Rosenberg6) first proposed the term 'sarcopenia.' Sarcopenia is an aging-associated condition defined as the loss of muscle strength due to loss of muscle mass. The diagnostic criteria for sarcopenia were presented by Baumgartner et al.7) in the 1998 New Mexico Elder Health Survey, but there is currently no generally accepted diagnostic method for sarcopenia. Studies on sarcopenia have made comparisons to osteoporosis, another typical physical change in the elderly, but studies of osteoporosis are lacking.8) Janssen et al.9) reported that the social cost associated with sarcopenia in the United States reached $18.5 billion in 2000, and noted the need for measures to address sarcopenia. The need for studies on and measures for sarcopenia is apparent in Korea as well, as it becomes an increasingly aging society.
Sarcopenia is associated with physical inactivity, disability, diabetes, metabolic syndrome, cardiovascular diseases, and mortality.10,11) Since depression is also linked to physical inactivity or dysfunction,12) there may be an association between sarcopenia and depression. The relationship between depression and obesity is well known. Meta-analyses have also the high probability that obesity accompanies and may be a risk factor for depression.13) In a study on sarcopenic obesity and mental health, Cho et al.14) also reported that sarcopenic obesity was associated with anxiety and depressive symptoms. Therefore, we speculated that sarcopenia and sarcopenic obesity would be associated with depression.
While recent studies have evaluated the association between sarcopenia and physical symptoms and diseases, studies on the association with mental health, including depression, are lacking. Although Kim et al.15) and Hsu et al.16) demonstrated that sarcopenia is associated with depression, additional studies are needed.
Studies on sarcopenia and depression to this point have been insufficient and few have included younger age groups. Therefore, the present study used data from the 2010ŌĆō2011 Korean National Health and Nutrition Examination Survey (KNHANES V-1, 2) to examine the relationship between sarcopenia and depression in the Korean population by age group and obesity status.
METHODS
1. Study Population
The KNHANES is conducted annually using a systematic sampling method after stratifying for population ratios based on the town units of dong, eup, and myun, as well as housing type and age group. The survey participants include household members at least one year of age from approximately 3,800 households nationwide. The first year of the fifth survey was conducted between January and December 2010; the second year continued from January to December 2011.17) The present study used data from 2010 and 2011; the most recent data that also included dual energy X-ray absorptiometry (DEXA). The present study included only those participants 20 years or older who had completed both the DEXA and the questionnaire. Participants with physician-diagnosed diseases that could also affect depression, such as cancer, liver cirrhosis, kidney failure, or cerebro- or cardiovascular diseases, were also excluded. The total study population was 7,364 individuals, comprised 5,245 and 2,119 people from 2010 and 2011, respectively, after excluding 1,420 and 4,381 of 6,665 and 6,500 adults for missing values. The present study used data from the KNHANES-V, which received institutional review board approval (2010ŌĆō02CON-21-C, 2011-02CON-06-C).
2. Measurement
1) Depressed state
As described previously,18) patients were classified as having depression, depressed symptoms, or not depressed. The depression group comprised respondents who indicated that they had been clinically diagnosed with depression. Among those who had not been clinically diagnosed as having depression, those who responded "yes" to the question "In the past year, have you felt sadness or despair continuously for two or more weeks that was severe enough to interfere with daily life?" were assigned to the depressed symptom group. Similarly, those who were not clinically diagnosed as having depression and who also did not report having experienced depressive symptoms for 2 weeks or more in the past year were categorized as not depressed.
2) Obesity and sarcopenia
Obesity was diagnosed using body mass index (BMI), with BMI Ōēź25 defined as obese when height (Ht) and weight (Wt) were substituted into the equation, BMI=Wt/Ht2.
Sarcopenia was diagnosed using a modified version of a method described in a previous study.19) After measuring participant appendicular skeletal muscle mass (ASM) via DEXA, the ASM/Wt (%) values were calculated; participants with values two standard deviations below the mean of the younger age group were classified as having sarcopenia.20) The mean ASM/Wt (%) of participants 20ŌĆō39 years of age, 26.88% for men and 21.02% for women, were used as the cut-off points. Depending on their sarcopenia and obesity status, the study participants were divided into sarcopenic obese, nonsarcopenic obese, sarcopenic nonobese, and nonsarcopenic nonobese groups.
3) Metabolic syndrome
Metabolic syndrome was diagnosed using the modified adult treatment panel III presented in 2005 by the American Heart Association and National Heart, Lung, and Blood Institute.21) Patients satisfying three or more of the five criteria listed below were considered to have metabolic syndrome: (1) waist size Ōēź90 cm for men and Ōēź85 cm for women;22) (2) triglyceride levels over 150 mg/dL or under treatment for hyperlipidemia; (3) blood pressure (BP) Ōēź130/85 mm Hg or under treatment for hypertension; (4) high density lipoprotein cholesterol levels (HDLC) <40 mg/dL for men and <50 mg/dL for women; and (5) fasting blood glucose levels over 100 mg/dL or under treatment for diabetes.
Serum triglyceride, HDLC, and fasting blood glucose levels were measured via an enzymatic method using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan).
3. Statistical Analysis
Because the number of subjects in the KNHANES varies from year to year, integrated weighted values were used for the analysis. Chi-square tests and analysis of variance were used to determine if the presence of sarcopenia was significantly associated with differences in depressed state. Stratified analysis was used to examine the association between sarcopenia and depression by age groups, while multiple logistic regression analysis was adjusted for covariates and performed to determine the relationship between sarcopenia and depression by gender. Gender, age, BMI, smoking, metabolic syndrome, diabetes, hypertension, and menopause (in women) were used as covariates. The statistical significance was set to <0.05. Categorical and continuous data were expressed as frequencies and means┬▒standard error. IBM SPSS Statistics for Windows ver. 22.0 (IBM Co., Armonk, NY, USA) was used for all statistical processing.
RESULTS
1. Clinical Characteristics of the Study Population
The mean ages in the sarcopenia and nonsarcopenia groups were 54.71 and 44.24 years, respectively, indicating a higher mean age among participants in the sarcopenia group. The sarcopenia group had higher total cholesterol, triglyceride, and low density lipoprotein cholesterol (LDLC) levels, but lower HDLC than the nonsarcopenia group. The prevalence of metabolic syndrome in the sarcopenia and nonsarcopenia groups was 58.7% and 25.3%, respectively. However, the difference in the prevalence of depressive symptoms and depression with sarcopenia between these groups was not statistically significant (Table 1).
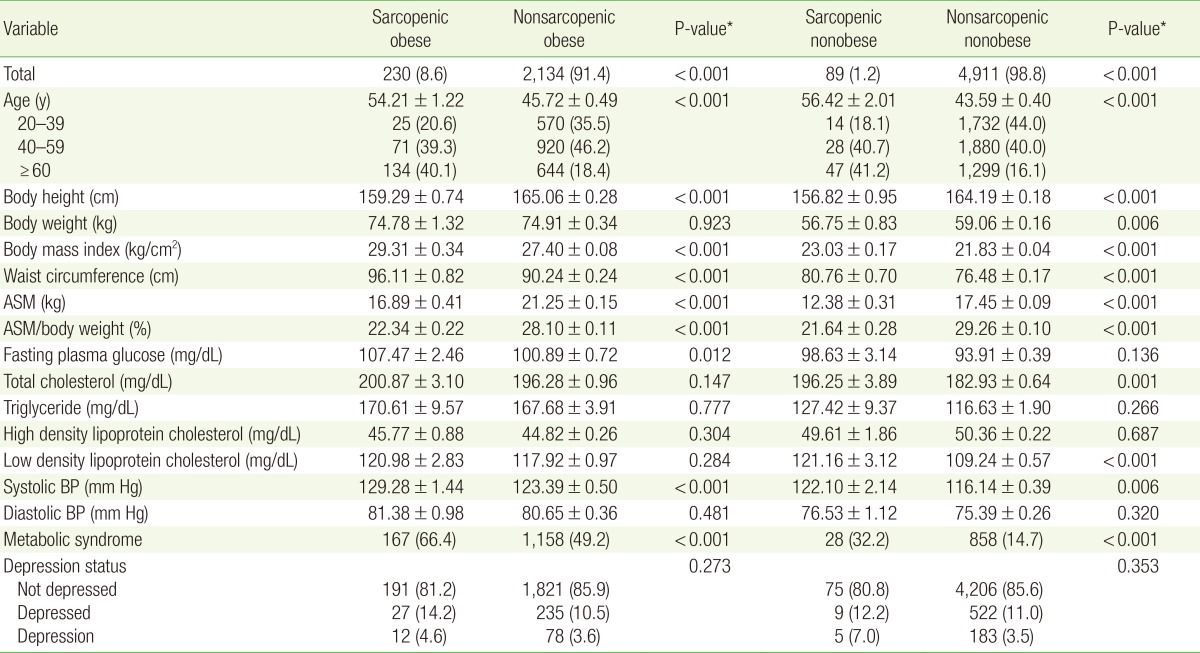
2. Depression by Sarcopenia and Obesity Status
The prevalence of sarcopenia in the obese and nonobese groups was 8.6% and 1.2%, respectively. Participants with sarcopenia who were also obese had higher systolic BP and prevalence of metabolic syndrome than the nonsarcopenic obese group. Meanwhile, the sarcopenic nonobese group showed higher levels of total cholesterol, LDLC, systolic BP, and prevalence of metabolic syndrome than the nonsarcopenic nonobese group; these findings suggest that, regardless of obesity status, sarcopenia was associated with higher systolic BP and prevalence of metabolic syndrome. Within the sarcopenic obese group, 14.2% had depressed symptoms, and 4.6% were depressed, compared to 10.5% and 3.6%, respectively, in the nonsarcopenic obese group. These results demonstrate that depressed symptoms and depression were higher in obese participants when accompanied by sarcopenia; however, these findings were not statistically significant. Similarly, depressive symptoms and prevalence of depression were higher in the sarcopenic nonobese group than in the nonsarcopenic nonobese group, again without statistical significance (Table 2).
3. Sarcopenia and Depression by Age Group
Stratified analysis was performed by age group after dividing the study population into four groups by sarcopenia and obesity status. Sarcopenia was not associated with depressive symptoms or prevalence of depression in any age group (20ŌĆō39, 40ŌĆō59, and Ōēź60 years) (Table 3).
4. Depression according to Sarcopenia Status
Multiple logistic regression analysis showed no association between sarcopenia and depression before and after adjusting for covariates. Moreover, sarcopenia was not associated with depression in either men or women (Table 4).
DISCUSSION
The present study used KNHANES V-1, 2 data to investigate the association between sarcopenia and depression. Although the sarcopenia group showed higher depressive symptoms and prevalence of depression than the nonsarcopenia group, the findings were not statistically significant. Sarcopenia was not associated with depression even in analyses that considered obesity status, age, and gender.
This study had several limitations. First, subjective judgment may influence the depression-related survey process. Koreans have a tendency to respond negatively to mental health-related questions. This tendency can lead to underestimation of the prevalence of depressive symptoms and depression, which may limit the informativeness of statistical testing. Second, classification errors are also possible since survey questions, rather than a specialized depression assessment tool, were used for classification. The relationship between two factors, therefore, might be underestimated due to the influence of non-discriminatory classification errors.
Previous studies have mostly reported associations between sarcopenia and depression in elderly men. Lee et al.23) reported that a decrease in skeletal muscles was associated with depressive symptoms in elderly Chinese men, while Kim et al.15) reported that sarcopenia was associated with depression in elderly Korean men. A study by Hsu et al.16) also reported sarcopenia to be associated with depression in Taiwanese veterans.
Although the mechanism of association between sarcopenia and depression has not been clearly identified, many factors have been suggested. Chronic low-level inflammation,24,25) excessive oxidative stress,26,27) and testosterone28,29) may be predictive factors for these diseases.
Unlike previous studies, the findings in the present study showed no association between sarcopenia and depression. While sarcopenia and depression share common factors, they have a weak influence on the association between these diseases. The typical physical changes in the elderly involve body composition changes, including increased body fat mass and weakening of the musculoskeletal system. The association between obesity, which is characteristic of body fat mass increase, and depression has been reported; however, the association between sarcopenia and depression remains inconsistent. Therefore, while the pathophysiology of depression is likely associated with an increase in body fat mass and adipose tissues, its association with a skeletal muscle decrease requires additional study. The scarcity of other studies on this topic, therefore, make the findings of the present study important for determining the criteria for associations between sarcopenia and other diseases.
The present study has several limitations. First, muscle strength or function was not considered when diagnosing sarcopenia. The diagnosis of sarcopenia based only on decreased skeletal muscle mass used in the present study may have resulted in errors in identifying participants with sarcopenia. Second, the cross-sectional nature of this study limited its ability to prove a causal relationship between sarcopenia and depression. Therefore, future longitudinal studies, including large-scale cohort studies, are necessary. Third, the use of a subjective questionnaire rather than a depression assessment tool to define the depressed state in this study could have led to underestimation and classification errors.
Despite these limitations, the present study is significant from the perspective that it used nationally representative data from KNHANES-V. The fact that the findings were contrary to previous studies is also meaningful. Future large-scale cohort studies on the association between sarcopenia and depression, as well as studies on the pathophysiology of sarcopenia, are necessary.