INTRODUCTION
There are five methods of obesity treatment: diet, exercise, behavior modification, drugs, and surgery. These treatment modalities can be divided into two categories, active and passive, based on the perspective of the patient. The active methods, including diet, exercise, and behavior modification, must be done by the patients themselves, whereas the passive methods of pharmacotherapy and bariatric surgery are performed by medical personnel.
A sufficient reduction in food intake and a radical increase in daily activity can reduce excess body weight and then maintain normal body weight in almost all patients with obesity. However, it is well established, through clinical experience and many previous clinical trials [1], that the standard active treatments are not strong enough to induce clinically significant weight loss. Very few patients with obesity can resist hunger and select low-energy-density foods when facing the excess availability of high-energy-density foods. Moreover, very few patients with obesity can maintain an active daily life given the present social prevalence of sedentary lifestyles. Thus, obesity specialists are constantly seeking passive methods of weight reduction.
Over the past decade, there have been major changes in the global treatment of obesity, and in Korea. Between 1964 and 2009, 25 antiobesity drugs, most of which were monoamine neurotransmitter reuptake inhibitors or releasers, were withdrawn after marketing in several countries or worldwide due to cardiotoxicity or potential for drug abuse/dependency [2]. Consequently, in 2009, orlistat was the only antiobesity drug approved for long-term treatment in Korea. However, Korean Ministry of Food and Drug Safety has approved three more antiobesity drugs for long-term management in the past decade and another drug is under consideration for approval. The currently prescribed anti-obesity drugs are listed in Table 1, along with their status in the controlled substances schedule, by the US Drug Enforcement Administration [3]. In addition, since 2019, bariatric surgery has been supported financially by the National Health Insurance Service.
In this review paper, the mechanisms of action and the clinical implications of the recently approved anti-obesity drugs, lorcaserin, naltrexone/bupropion, and liraglutide, will be described.
MECHANISM OF ACTION OF CENTRALLY ACTING ANTI-OBESITY DRUGS
In the previous era of anti-obesity drugs, it was unclear how the centrally acting anti-obesity drugs suppressed appetite; however, the mechanism of action of orlistat, a gastric/pancreatic lipase inhibitor that inhibits the absorption of dietary fat in the small intestine, was well characterized. However, the appetite-suppressing mechanisms of lorcaserin, naltrexone/bupropion, and liraglutide are easy to understand. Before the mechanism of action of anti-obesity drugs is described, a brief overview of the mechanism of energy homeostasis in the brain will be provided.
1. Energy Homeostasis and the Arcuate Nucleus
For the maintenance of energy homeostasis, it is essential to sense the peripheral signals related to the amount and accessibility of energy. The signals can be divided into two groups: the relatively stable signals that describe the amount of overall stored energy in the body; and the rapidly changing signals that describe the sudden energy consumption, the recent food intake, food availability, and anticipated energy consumption. These peripheral signals of body energy status are considered to be transferred to a specific region of the brain through the humoral and neural pathways and are integrated there. The signaling routes for the control of obesity have been described in detail previously [4].
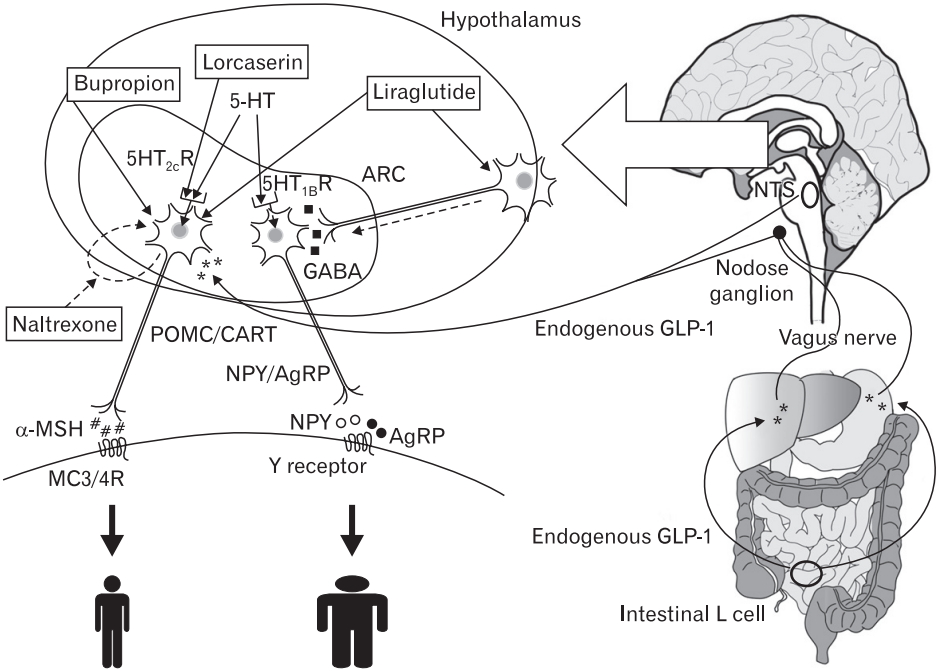
The neurons in the arcuate nucleus of the hypothalamus, which control food intake and energy expenditure, can be grouped into two major populations: orexigenic neurons, which express neuropeptide Y (NPY) and/or agouti-related peptide (AgRP); and anorexigenic neurons, which express proopiomelanocortin (POMC) and/or cocaineand amphetamine-regulated transcript (CART). These two neuron populations gather and integrate the peripheral signals related to the current energy status of body, the presence of food, and the amount of food intake, and they activate the feeding center or transmit signs of satiety, which stop feeding behavior and suppress feeding actions for a certain period of time. Downstream of the POMC/CART neurons, the activation of melanocortin (MC) 3 and 4 receptors by α-melanocyte stimulating hormone occurs (Figure 1).
2. Serotonergic Satiety in Brain
Serotonin (5-hydroxytryptophan, 5-HT) is a monoamine neurotransmitter that is been well conserved across species throughout evolution [5]. The 5-HT system and receptors are quite varied and the 5-HT receptors have been grouped into seven families, 5-HT1 to 5-HT7, which include 14 known subtypes [5]. 5-HT is involved in diverse physiology, including cognition, mood, sexual behavior, and feeding behavior [5].
Although 5-HT has been conserved well throughout evolution, 5-HT systems are different in invertebrate animals and mammals. Although 5-HT neurons are broadly distributed throughout the CNS in lophotrochozoan invertebrates, they are concentrated largely in the raphe nucleus in mammals [6]. The role of 5-HT in eating behavior is not the same in invertebrates and mammals. In invertebrate animals, 5-HT promotes feeding behavior, whereas in mammals, its main role is in the induction of satiety [6].
For the investigation of the involvement of 5-HT receptor subtypes in satiety, several compounds that differ in their affinity to the receptor subtypes have been used, including m-chlorophenylpiperazine (mCPP), RU-24969, 1-(3-trifluoromethylphenyl) piperazine (TFMPP), and 2,5-dimethoxy-4-iodoamphetamine (DOI) [7]. According to the reports investigating mCPP, RU-24969, TFMPP, and DOI, of the various 5-HT receptors, 5-HT1B and 5-HT2C are predominantly involved in satiety [7].
3. Interaction of Serotonin Satiety System with POMC/CART Neurons and NPY/AgRP Neurons
The anorexic effects of the serotonin receptor agonist (RA), fenfluramine, which was widely administered to patients with obesity in the early 1990s, were known to be mediated through the central melanocortin system [8]. Lam et al. [9] reported that 5-HT2C receptors were expressed on POMC neurons, and prolonged infusion with BVT.X, a selective 5-HT2C RA, significantly increased the expression of POMC mRNA, which was not observed in MC4 receptor knockout mice. The MC3 receptor was reported to be more likely downstream of serotonin-induced hypophagia, through a study of MC3 knockout, MC4 knockout, and MC3/MC4 double knockout mice [10]. Moreover, the systemic administration of fenfluramine can acutely suppress the expression of NPY in hypothalamic neurons, although the expression returns to normal with chronic administration [11,12]. 5-HT1B RAs were shown to hyperpolarize NPY neurons, whereas 5-HT1B receptor antagonists prevented the hyperpolarization induced by 5-HT1B RAs [13]. These findings suggested that 5-HT may directly inhibit NPY/AgRP neuron activity through the inhibitory 5-HT1B receptor.
In conclusion, 5-HT suppresses NPY/AgRP neurons, but stimulates POMC/CART neuron through the 5-HT1B and 5-HT2C receptors, and these effects are transferred to the MC3/4 receptors to induce hypophagia (Figure 1).
4. Gut to Brain
Preproglucagon, coded by the proglucagon gene, is processed to glucagon-like peptide-1 (GLP-1), and is secreted from intestinal endocrine L-cells, which are located mainly in the distal ileum and colon, and preproglucagon-expressing neurons in the nucleus tractus solitarius (NTS) of the brain stem [14,15]. Although there are many GLP-1 binding sites in the brain, the half-life of endogenous GLP-1 secreted from the gut is too short to reach the brain owing to the rapid degradation; this occurs mainly through dipeptidyl peptidase-4 (DPP-4) and DPP-4 shortens the half-life of GLP-1 to several minutes. However, unlike gutderived endogenous GLP-1, GLP-1 RAs have a much longer half-life owing to their resistance to degradation by DPP-4, conferred by their structural differences, including changes in the amino acid sequence; therefore, some GLP-1 RAs may reach the brain through the humoral pathway, cross the blood-brain barrier (BBB), and attach to GLP-1 binding sites in the brain. GLP-1 RAs that reach the inside of brain may act like brain-derived endogenous GLP-1.
GLP-1 can activate the hepatic vagal nerve and the vagal afferent fibers of nodose ganglion neurons [16,17]. In rats with subdiaphragmatic vagal deafferentation, the hypophagic effect of intraperitoneally injected GLP-1 was suppressed in the early stage (until 1 hour) of low-dose administration, whereas the hypophagic effect was observed in the later stages (≥2 hours) or by a high-dose administration [18]. Similarly, the hypophagic effect of liraglutide was sustained in rats with subdiaphragmatic vagal deafferentation[19]. According to these findings, putatively, the neural pathway through the vagus nerve is responsible for a large part of the influence of endogenous gut-derived GLP-1 on the brain, whereas peripherally administered long-acting GLP-1 RAs act directly on brain GLP-1 RAs through the humoral pathway.
5. Mechanisms of Action of Lorcaserin and Liraglutide
Considering the energy homeostasis mechanism described above, the action mechanism of lorcaserin, a selective 5-HT2C RA, is very clear: it stimulates POMC/CART neurons, which results in the activation of MC3/4 receptors.
However, the weight-reducing mechanism of liraglutide requires further explanation. A well-known effect of gut-derived endogenous GLP-1 is the inhibition of gastric emptying, which is related to the main side effect of liraglutide, nausea. However, the weight loss effect of liraglutide does not appear to depend on the delay in gastric emptying, at least in rats. The chronic administration of the long-acting GLP1 RA liraglutide induces desensitization of gastric inhibition, whereas the short-acting GLP-1 RA exenatide does not [20]. This is the reason for stepwise up-titration in the administration of liraglutide to the patients.
The hypophagic effect of liraglutide does not rely on the neural pathway through the vagus nerve, and it is independent of GLP-1 receptors in the area postrema and the paraventricular nucleus [19]. Liraglutide does not activate endogenous GLP-1-producing neurons in the NTS [19]. However, liraglutide acts directly on POMC/CART neurons and NPY/AgRP neurons. Liraglutide increases the expression of POMC mRNA, but does not affect the expression of CART mRNA.19) In the comparison of weight-matched rats, liraglutide-treated rats showed lower expression of NPY mRNA and AgRP mRNA, indicating that liraglutide suppressed the elevation of food-deprived hunger signals [19]. However, there are no GLP-1 receptors on NPY/AgRP neurons, and the inhibitory signal of liraglutide on orexigenic NPY neurons is transmitted via γ-aminobutyric acid (GABA)-dependent signaling [19]. In addition, the activation of GLP-1 receptors suppressed the reward system activity of mesolimbic dopamine neurons to highly palatable food intake, which may be a mechanism through which liraglutide demonstrates its hypophagic effect [21].
GLP-1 can induce direct thermogenesis. It was demonstrated that GLP-1 increased thermogenesis in rats, mediated by the lower brainstem and the sympathoadrenal system, with a larger increase observed from intravenous administration than from intracerebroventricular administration [22]. The thermogenic effect of GLP-1 is induced by the increase in interscapular brown adipose tissue activity, which depends on adrenergic signaling [23]. However, the increase in resting energy expenditure was not significant in patients with type 2 diabetes mellitus (T2DM) [24).
In conclusion, the hypophagic effect of liraglutide depends on the direct activation of POMC/CART neurons and the indirect suppression of NPY/AgRP neurons through GABA-dependent signaling, and the suppression of mesolimbic dopamine reward system (Figure 1). The weight loss results of clinical trials of lorcaserin and GLP-1 RAs are summarized in Tables 2 and 3, respectively [25-32].
6. Combination of Naltrexone/Bupropion
The fixed dose drug combination of sustained-release (SR) naltrexone 32 mg and SR bupropion 360 mg (NB) is one of the approved antiobesity drugs for long-term treatment in Korea.
In the arcuate nucleus, dopamine receptor activation suppresses NPY neurons and stimulates POMC neurons, most likely through D2 receptors [33,34]. The intraperitoneal co-administration of a selective dopamine reuptake inhibitor with a selective norepinephrine reuptake inhibitor showed additive effects on negative energy balance in mice [35]. Although bupropion, a norepinephrine-dopamine reuptake inhibitor, is unique among anti-depressants owing to its association with weight loss due to its mechanism of action, the extent of weight reduction from bupropion is minimal in patients with obesity. In a randomized placebo-controlled trial, 24-week administration of SR bupropion 300 and 400 mg/d were associated with mean weight loss of 5.7% and 7.7%, respectively, compared with that of 4.0% in the placebo group [36].
Naltrexone, an opioid receptor antagonist used in the treatment of opioid or alcohol dependence, resulted in the dose-related suppression of eating and drinking in rats [37]. Consequently, naltrexone was administered to patients with obesity in several clinical trials in the 1980s to induce weight loss in humans, but the results were unsuccessful [38,39].
Although the weight loss effects of bupropion and naltrexone in humans were not satisfactory, in vivo electrophysiology studies by Greenway et al. [40] demonstrated that bupropion stimulated POMC neurons and the combination of bupropion and naltrexone showed greater effects on POMC neurons. Animal studies, preclinical, and clinical trials of NB showed that this combination had a greater weight loss effect compared with previous results for the monotherapy of each drug [40-44]. In conclusion, the mechanism of action of NB is the stimulation of POMC neurons with bupropion, with this stimulation augmented by blocking of the autoinhibitory mechanism of POMC by naltrexone (Figure 1). The weight loss results of clinical trials of NB are summarized in Table 2 [41-44].
GLP-1 RECEPTOR AGONISTS FOR THE TREATMENT OF OBESITY: LIRAGLUTIDE AND SEMAGLUTIDE
Presently, six GLP-1 RAs are used worldwide for the treatment of T2DM: albiglutide, dulaglutide, exenatide, liraglutide, lixisenatide, and semaglutide. Except for semaglutide, these GLP-1 RAs have been approved in Korea. Although the six GLP-1 RAs share a mechanism of action and their basic characteristics, there are differences among the drugs. The detailed similarities and differences of these drugs are beyond this review and are were described [45]. Essentially, the GLP-1 RAs can be categorized by their duration of action for the stimulation of the GLP-1 receptor in circulation: short-acting (exenatide and lixisenatide) and long-acting (albiglutide, dulaglutide, exenatide long-acting release, liraglutide, and semaglutide). The main mechanism of the glucose-lowering effect is somewhat different between the two groups. The short-acting GLP-1 RAs inhibit gastric emptying and mainly lower postprandial glucose levels, whereas the long-acting drugs stimulate postprandial insulin secretion and suppress fasting glucagon secretion, which can affect both fasting and postprandial blood glucose levels [45,46].
Endogenous GLP-1, liraglutide, and lixisenatide can cross the BBB and reach the hypothalamus [19,47,48]. However, there is no evidence that other GLP-1 RAs cross the BBB. The molecular size and structure of albiglutide and dulaglutide are completely different from endogenous GLP-1; therefore, it is difficult for them to cross BBB and act on the hypothalamic neurons through the humoral pathway.
Of the six GLP-1 RAs, only liraglutide and semaglutide were researched for long-term weight management; liraglutide is currently available in Korea. There have been several large phase 2 and 3 clinical trials for these drugs in the treatment of obesity and the participants and mean weight loss results are summarized in Table 3 [28-32]. As shown in the clinical trials, the weight reduction effect of liraglutide was modest (mean weight loss from -5.7% to -8.0%) and that of semaglutide was strong (-17% for rapid dose escalation of 0.4 mg). Unlike liraglutide, semaglutide can be administered orally. Oral semaglutide in a tablet form is co-formulated with the absorption enhancer sodium N-[8 (2-hydroxybenzoyl) amino] caprylate. In a clinical trial of daily administered oral semaglutide (2.5 to 40 mg) for 26 weeks in patients with T2DM, the dose-dependent range in the reduction of hemoglobin A1c induced was -0.7% to -1.9%, whereas those induced by 1 mg weekly administered semaglutide through the subcutaneous route and oral placebo were -1.9% and -0.3%, respectively [49]. In that trial, the weight reduction in oral semaglutide for each dosage was as follows: placebo, -1.2 kg; 2.5 mg group, -0.9 kg; 5 mg group, -1.5 kg; 10 mg group, -3.6 kg; 20 mg group, -5.0 kg; 40 mg standard escalation group, -5.7 kg. Thus, subcutaneous injection is better than per oral administration for semaglutide. The mainstream obesity treatment of GLP-1 RAs will move to semaglutide from liraglutide in the near future, considering the results of clinical trials. Putatively, in some areas, bariatric surgery can be replaced with semaglutide.
Beyond obesity treatment, liraglutide has some other potential clinical uses. Patients with schizophrenia have high mortality rate; one of the primary causes of their death is cardiovascular disease [50]. Although anti-psychotic drugs are effective for the treatment of schizophrenia, they induce weight gain and adverse metabolic effects in patients with schizophrenia [51]. In a small clinical trial, liraglutide improved glucose tolerance and reduced body weight in patients with schizophrenia spectrum disorders on clozapine or olanzapine [52].
Bariatric surgery induces a large weight reduction in patients with morbid obesity and substantial remission of T2DM. However, T2DM relapses occurred in a considerable number of the patients with diabetes who achieve remission through surgery [53]. Small-scale retrospective reports suggested that liraglutide could be an option for patients who experienced poor weight loss or weight regain after bariatric surgery [54,55].
Although liraglutide was not approved for patients under 18 years of age in Korea, a randomized controlled 5 week trial of 21 adolescents between 12 and 17 years of age reported that the administration of liraglutide resulted in similar safety and tolerability as administration to adults [56].
CARDIOVASCULAR SAFETY OF ANTI-OBESITY DRUGS
Diabetes is diagnosed from an elevated blood glucose level and nonenzymatic glycation products; thus, the tight control of blood glucose should be the core of the prevention of cardiovascular disease, which is the most common cause of mortality, disability, and financial burden. However, intensive glycemic control was shown to fail in the reduction of macrovascular episodes, even though it reduced microvascular events in well-known large clinical observational or interventional studies [57].
It is certain that obesity increases cardiovascular risk and that weight reduction can ameliorate risk. However, similar to the glycemic control achieved with anti-diabetic drugs, there is little evidence on whether the weight reduction induced by anti-obesity drugs can decrease or postpone cardiovascular events in patients with obesity. Conversely, several anti-obesity drugs, including fenfluramine and sibutramine, were banned from market owing to their deleterious effects on the cardiovascular system [2]. Based on these historical events, newly developed anti-obesity drugs should have proven safety and/or efficacy on cardiovascular events in addition to its weight loss effect.
In the past several years, three clinical trials of the cardiovascular safety of anti-obesity drugs have been performed: the CAMELLIA-TIMI 61 [58] trial of lorcaserin, the study by Nissen et al. [59] of NB, and the LEADER trial of liraglutide in patients with T2DM [60]. The results of the trials are summarized in Table 4. In the lorcaserin group, there was no increase in the risk of cardiovascular events during the trial. The liraglutide group (administered up to 1.8 mg daily for the treatment of diabetes) had lower rates of cardiovascular events and all-cause death than the placebo group, although there were no significant differences between the liraglutide and placebo groups with respect to myocardial infarction and for stroke. However, the safety of NB for cardiovascular events was not confirmed, because trial was terminated prematurely owing to early data release. In addition, the cardiovascular safety or efficacy of the higher dosage of liraglutide (3.0 mg) for the treatment of obesity has not yet been studied.
Of these three trials, the major cardiovascular events and all-cause death rates were clearly higher in the liraglutide trial (LEADER); this may have been because the proportion of patients with diabetes, the proportion of established cardiovascular disease, and the level of glycated hemoglobin were higher. The lack of cardiovascular benefits in the clinical trials of anti-obesity drugs may be a result of: (1) insufficient length of the study; (2) the moderate cardiovascular risk of participants; and (3) the usage of anti-hypertensive agents, statins, or antiplatelet agents.
CONCLUSION
Lorcaserin stimulates POMC/CART neurons and inhibits NPY/AgRP neurons, which results in the activation of the MC3/4 receptors. The mechanism of action of NB is the stimulation of POMC neurons with bupropion, augmented with blocking of the autoinhibitory mechanism of POMC by naltrexone. The hypophagic effect of liraglutide depends on its direct activation of POMC/CART neurons and the indirect suppression of NPY/AgRP neurons through GABA-dependent signaling, with adjunctive suppression of the mesolimbic dopamine reward system. Among GLP-1 RAs, semaglutide is expected to be added to the list of anti-obesity drugs in the near future. In patients with obesity patients with high cardiovascular risk, lorcaserin was neutral and liraglutide (up to 1.8 mg) was favorable, whereas the results of NB were inconclusive.