INTRODUCTION
Diverticular disease along the esophagus, stomach, and small bowel can present in many ways. Diverticula found within the stomach are usually asymptomatic and many are found incidentally during evaluation for other reasons. On the other hand, diverticula found within the esophagus such as Zenker’s diverticulum, usually present with symptoms such as dysphagia, regurgitation, and aspiration. Asymptomatic diverticula do not necessarily require treatment. However, those that do cause symptoms will likely require intervention to improve the quality of life of those affected. This article reviews the various diverticula found along the foregut and small bowel, with emphasis on the pathophysiology, clinical presentation, and treatment for the diseases.
ESOPHAGUS
1. Zenker’s Diverticulum (Figure 1)
Zenker’s diverticulum is an outpouching at the level of the pharynx through the Killian’s triangle, bordered by the thyropharyngeus and cricopharyngeus of the inferior pharyngeal constrictor muscle, due to dysfunction of the cricopharyngeal muscle [1]. This condition is the most common in elderly men [2].
1) Pathophysiology
The cricopharyngeus of the inferior pharyngeal constrictor muscle fails to relax, resulting in increased intraluminal pressures proximal to the obstruction, which results in protrusion of the mucosa and submucosa through the esophageal wall [3].
3) Treatment
Treatment focuses on relieving the pressure distal to the diverticulum using cricopharyngeal myotomy. Surgical management includes endoscopic diverticulotomy as opposed to operative myotomy with or without diverticulectomy or diverticulopexy [5]. Carbon dioxide laser and stapler-assisted techniques are the two main endoscopic treatment modalities [5,6]. Endoscopic management has gained popularity, as it is minimally invasive, and the patient population with this condition is typically elderly with likely multiple medical comorbidities [3]. Both open surgery and endoscopic management are considered safe and effective [1,2,7]. Endoscopic management offers shorter operative time and hospital stay; however, similar time to initiation of oral diet can be achieved in both patients treated with endoscopy and those treated with open surgery [2,4,5]. The durability of repair is higher among patients who undergo open surgery [1,4].
2. Traction Diverticulum (Figure 2)
Traction diverticulum is a true diverticulum most often caused by inflammatory processes in the mediastinum that usually present in the mid esophagus [8].
1) Pathophysiology
Traction diverticulum develops because of focal traction in a region of inflammatory process within the mediastinum most commonly associated with granulomatous disease [3].
2) Clinical presentation
Patients with traction diverticulum are usually asymptomatic and diagnosed incidentally during an imaging examination such as an esophagram obtained for other reasons [3].
3) Treatment
In cases of large diverticula, a diverticulectomy or diverticulotomy may be performed. An esophagogastric myotomy may be performed with diverticulectomy to decrease the risk of staple line leak [3]. The surgical management of asymptomatic patients with small diverticula is controversial [8]. A trial of close observation is an option in this subgroup of patients.
3. Pulsion Diverticulum (Figure 3)
Pulsion diverticulum is a false diverticulum that results from an increased intraluminal pressure that causes the mucosal and submucosal layers to protrude through a focal area of the esophageal wall [8]. An epiphrenic diverticulum is a subtype of pulsion diverticulum that occurs in the distal 10 cm of the esophagus [9,10]. Most pulsion diverticula occur in the epiphrenic region [8].
1) Pathophysiology
Pulsion diverticulum is due to functional obstruction resulting from esophageal motility disorders such as achalasia or diffuse esophageal spasm [8,10,11]. The disorganized contraction within the esophagus results in increased intraluminal pressures, which lead to the outpouching of the mucosal and submucosal layers [8,10].
2) Clinical presentation
Patients with an epiphrenic pulsion diverticulum present with dysphagia, regurgitation, chest pain, heartburn, aspiration, and aspiration pneumonia [10]. Patients with mid-esophageal pulsion diverticulum may present with dysphagia, intermittent emesis, and substernal chest pain [11]. The size of the diverticulum does not correlate to the severity of symptoms [9].
3) Treatment
The most common treatment for epiphrenic pulsion diverticulum consists of diverticulectomy combined with cardiomyotomy or a more limited myotomy followed by partial fundoplication such as Dor or Toupet fundoplication. Myotomy is performed to prevent the uncoordinated esophageal contractions. Diverticulectomy has been questioned as a necessary procedure, as patients who underwent cardiomyotomy and partial fundoplication without diverticulectomy had no significantly different outcomes. Laparoscopic and thoracoscopic techniques are more commonly used than open techniques [8,10]. Both techniques have similar outcomes and complication rates, although minimally invasive techniques are associated with a shorter length of hospital stay and lower 30-day mortality rates [8,9]. In the treatment for mid-esophageal pulsion diverticulum, thoracoscopic techniques would need to be performed because these allow for a better access to the diverticulum. A partial fundoplication may not be necessary if the lower esophageal sphincter is not violated during myotomy [11].
STOMACH
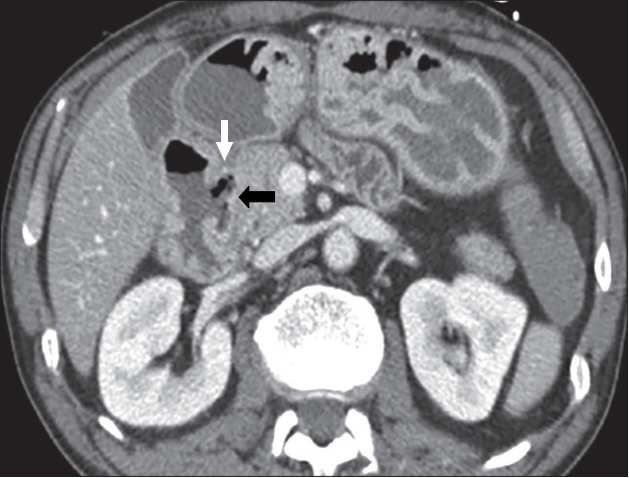
1. Gastric Diverticulum (Figure 4)
Gastric diverticulum can present as either congenital or acquired [12]. Congenitally acquired gastric diverticulum is a true diverticulum and is most commonly located near the gastroesophageal junction along the posterior wall or lesser curvature [13-16]. Acquired gastric diverticulum is usually a false diverticulum and is usually located in the distal one-third of the stomach, near the pylorus [12,14,15]. Gastric diverticula are rarely found along the greater curvature [17].
1) Pathophysiology
Congenital gastric diverticulum is a result of malformation or interrupted development of the stomach during the fetal period [17]. Acquired gastric diverticulum develops as either traction or pulsion diverticulum [12,15]. Gastric diverticulum arising as traction diverticulum can be due to other disease processes that cause increased intraluminal pressures, such as pyloric obstruction, severe vomiting, coughing, or foreign bodies [15,17]. Pulsion diverticulum, similar to that found in the esophagus, results from nearby inflammatory processes that cause adhesive forces that lead to outpouching [12,15,17].
2) Clinical presentation
Gastric diverticulum is usually asymptomatic and found incidentally [16]. Symptomatic patients may present with a sensation of fullness or pain in the left upper abdomen after meals, dyspepsia, vomiting, or halitosis [12,15]. A lack of pathognomonic symptoms makes the diagnosis of the condition certainly difficult [18].
3) Treatment
Asymptomatic cases can be observed without further treatment [15,17,18]. Nonoperative management of mildly symptomatic gastric diverticulum includes the use of proton pump inhibitors, antacids, and antispasmodics [12,15,17,18]. Surgical management involves resection of the diverticulum via primary repair and is indicated in large symptomatic cases or symptomatic cases not relieved using medical therapy [15,17-19].
DUODENUM
1. Duodenal Diverticulum (Figure 5)
Duodenal diverticulum is an outpouching of the duodenum and can be congenital or acquired [20,21]. Congenital diverticulum can be found anywhere along the duodenum. The acquired type is more common than the congenital variant and usually present along the medial wall of the second and third segments of the duodenum [20]. The duodenum is the second most common location for diverticula after the colon [22]. The condition is more common in women and the elderly [20].
1) Pathophysiology
Congenital diverticulum is a true diverticulum and likely arises from maldevelopment of the primitive foregut [20]. An intraluminal subtype arises from a spectrum of duodenal recanalization disorders where a web progressively elongates due to normal duodenal peristalsis [22]. Acquired diverticulum is a false diverticulum of the pulsion type from increased intraluminal pressures due to mechanical obstruction or uncoordinated contraction [20,21].
2) Clinical presentation
Patients with duodenal diverticula are usually asymptomatic and, consequently, diagnosed incidentally on imaging or endoscopy [20,23]. Diverticula can cause symptoms if they become perforated or inflamed, or if hemorrhage occurs [23]. Diverticulitis is an uncommon condition given the relative sterile environment of the duodenum. Perforation of the diverticulum from extensive inflammation, enterolithiasis, ulceration, foreign body, trauma, iatrogenic causes, or ischemia from distention due to retained food contents can result in abscess formation, fistula to surrounding organs, or obstruction of the common bile duct [21]. If the diverticulum arises in the juxtapapillary or periamullary region, the ampulla and distal common bile duct may be compressed, which leads to symptoms of jaundice, biliary cholangitis, or right upper quadrant pain from biliary calculus [20].
3) Treatment
Asymptomatic cases may be treated conservatively with observation. In cases of perforated duodenal diverticulum with minimal-to-mild inflammation, diverticulectomy is performed via the single- or double-layer closure of the duodenum followed by drainage of any residual fluid collection [23]. Other approaches for patients with mild symptoms who are poor surgical candidates include nonoperative management with intravenous antibiotics, bowel rest, nasogastric tube decompression, and percutaneous drainage of fluid collections [21]. If extensive inflammatory changes occur, primary closure of the duodenum may not be possible, and a Whipple procedure may be indicated [21]. Owing to the rarity of this condition, no standardized treatment protocol has been established [21,23].
JEJUNUM AND ILEUM
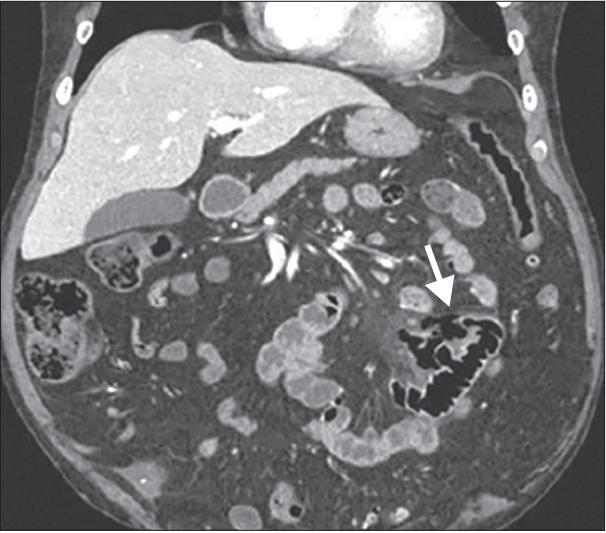
1. Jejunoileal Diverticulum (Non-Meckelian) (Figure 6)
Diverticula found in the jejunum and ileum are rare [24,25] and can be either congenital or acquired [24]. This condition is more common among men and is typically found in the sixth or seventh decades of life [26]. Diverticula tend to occur along the mesenteric border of the intestine and are found in multiples more proximally in the small bowel and solitarily in the distal ileum [24,26].
1) Pathophysiology
Small bowel diverticula are thought to arise from abnormal contractions that lead to increased intraluminal pressures [24,26]. As such, most diverticula are thought to be of the acquired pulsion type [26]. Neurological conditions such as myasthenia gravis are thought to be associated with the development of diverticula, as these conditions predispose to abnormal contractions within the bowel [25]. Diverticula usually occurs at the site of the intestinal arteries penetrating the intestinal muscular layer [26]. The higher incidence of diverticula in the jejunum than in the ileum is likely due to the larger size of the penetrating intestinal arteries in the jejunum [25].
2) Clinical presentation
Most patients with jejunoileal diverticula are asymptomatic [24,25]. In the few symptomatic cases, patients may present with abdominal pain, nausea, vomiting, anorexia, weight loss, or flatulence [24]. More serious complications include acute diverticulitis, bowel obstruction, traumatic rupture, and volvulus. Small bowel diverticula may also present with hematochezia or melena if a perforating intestinal artery with inflammatory process is involved [25].
3) Treatment
Asymptomatic cases are managed conservatively [25]. Symptomatic or complicated cases of small bowel diverticula are resected with primary anastomosis [24,25]. Given that diverticula arise from the mesenteric side of the bowel, primary closure may not be possible, and segmental resection is recommended [26].
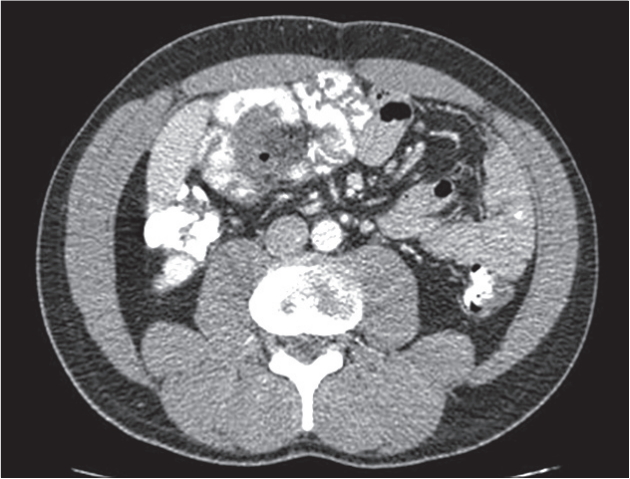
2. Meckel’s Diverticulum (Figure 7)
Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract [27-31]. It is found in 2% of the population with symptomatic cases having a male-to-female predominance of 2:1 to 5:1 [28,29,32]. Its prevalence in asymptomatic cases does not significantly differ between the sexes [32]. These diverticula are most commonly found 40–100 cm proximal to the ileocecal valve [27,29-31].
1) Pathophysiology
Meckel’s diverticulum arises from the anti-mesenteric side of the ileum because of incomplete obliteration of the omphalomesenteric duct [27-31]. It is a true diverticulum involving all three layers of the bowel wall [27]. Ectopic mucosa can be found in Meckel’s diverticulum, with gastric mucosa being the most common [27-29]. Less commonly found is ectopic mucosa of pancreatic, duodenal, colonic, endometrial, or hepatobiliary origin [27,28,31].
2) Clinical presentation
Most patients with Meckel’s diverticulum are asymptomatic [30,31]. The most common clinical presentation among pediatric patients is painless rectal bleeding due to erosion of the bowel mucosa by acid-secreting ectopic gastric mucosa [27,28,31]. The higher prevalence of symptomatic cases among men is hypothesized to be due to the increased acidsecreting ability within the larger parietal cells [32]. For patients presenting with bleeding, the most sensitive test to detect Meckel’s diverticulum is a nuclear medicine Meckel’s scan (technetium-99m pertechnetate scintigraphy), as it is taken up by parietal cells in the ectopic gastric mucosa [27,28,30,31]. Small bowel obstruction is the second most common presentation of Meckel’s diverticulum in the pediatric population, while this is the most common presentation in adults [27]. Meckel’s diverticulum can also perforate and result in peritonitis mimicking acute appendicitis [28]. Inflammation of the diverticulum can result in diverticulitis and ulceration [32]. Symptomatic presentation of Meckel’s diverticulum decreases with age, mostly occurring before 10 years of age, with 42% of patients aged <2 years [27,32].
3) Treatment
Symptomatic Meckel’s diverticulum is managed with open or laparoscopic resection of the diverticulum with possible resection of the adjacent bowel if vascular compromise is found in the setting of bowel obstruction [27-29]. Diverticulectomy alone is sufficient in cases of bleeding in Meckel’s diverticulum, as it was shown to have similar outcomes as diverticulectomy with bowel resection [29]. Incidentally found Meckel’s diverticulum during imaging or surgical procedures performed for other reasons can be managed with close observation alone [27,31]. The appearance of Meckel’s diverticulum during surgery does not indicate the presence of ectopic gastric mucosa [28].
CONCLUSION
Diverticular disease found within the esophagus usually present with symptoms related to disruption of normal esophageal motility such as dysphagia, regurgitation, and aspiration. Contrary to esophageal diverticula, diverticular disease of the stomach and small bowel are usually asymptomatic and are found incidentally. Asymptomatic diverticula can be managed with observation alone. In symptomatic cases, patients may be referred for endoscopic or surgical treatment, depending on the severity of the symptoms.