INTRODUCTION
Hypothyroidism is a significant health problem that increases in frequency in the elderly. It affects approximately 4.6% of the US population (overt hypothyroidism, 0.3%; subclinical hypothyroidism, 4.3%) and 3.8% of the Korean population (overt hypothyroidism, 0.7%; subclinical hypothyroidism, 3.1%) [1,2]. The frequency of subclinical hypothyroidism increases in older adults, affecting approximately 6% of individuals aged 70–79 years and 10% of individuals aged 80 years or older [3]. The clinical manifestations of hypothyroidism include dry skin, cold sensitivity, fatigue, muscle cramps, voice changes, and constipation [4]. Hypothyroidism in the elderly also causes atypical symptoms, which include gustatory changes, hearing loss, and ataxia.
While the increased prevalence of hypothyroidism in the elderly is accompanied by higher rates of physical and cognitive impairments, depression, and cardiovascular diseases, hypothyroidism may have a protective health effect in older adults [3,5-9]. While reports differ, some studies have shown that older adults with thyroid stimulating hormone (TSH) levels that correspond to mild to overt hypothyroidism may have better mobility and slower decline in measures of physical function than their euthyroid counterparts [3,6]. Further, studies have shown that subclinical hypothyroidism in the elderly is not associated with depression or cognitive impairment [6,10,11].
To date, only a few studies have investigated the association between various degrees of hypothyroidism and measures of health-related quality of life in geriatric populations. The Korea National Health and Nutrition Examination Survey (KNHANES) represents a large and reliable dataset based on a nation-wide survey. Given the lack of studies that investigate the health effects of different thyroid statuses in geriatric populations and the importance of verifying their association, we assessed the cross-sectional relationship between thyroid status and EuroQol-5 dimension three-level version (EQ-5D-3L) utility values using data from the sixth KNHANES conducted from 2013 to 2015.
METHODS
1. Study Population and Data Collection
This study was conducted using data from the sixth KNHANES, a national cross-sectional survey conducted by the Korea Centers for Disease Control and Prevention for Health Statistics. The KNHANES is an independent dataset from the general South Korean population, similar to the National Health and Nutrition Examination Survey conducted by the US Centers for Disease Control and Prevention [12]. The selection process of household units and participants for the KNHANES is based on a stratified, multi-stage, clustered probability sampling design to represent the noninstitutionalized Korean population. The health interview includes the use of an established questionnaire to determine the demographical information of the subjects and basic laboratory data. In the sixth KNHANES (2013–2015), laboratory measurements of serum TSH, free T4 (fT4), and thyroid peroxidase antibody (TPO Ab) were obtained using subsampling stratified by sex and age. Approximately one-third of subjects aged over 10 years among a total of 2,400 individuals annually were selected by subsampling considering sociodemographic factors to undergo thyroid function tests.
Among the 1,195 subjects aged over 60 years who participated in the sixth KNHANES and underwent thyroid function tests, the following were excluded: those with missing EQ-5D-3L utility values (n=74); those with self-reported history of thyroid diseases, including thyrotoxicosis, overt hypothyroidism, benign thyroid nodules, and Hashimoto’s thyroiditis, and those who were on treatment for thyroid diseases, including radioactive iodine treatment, antithyroid drugs (propylthiouracil, methimazole, and carbimazole), and thyroid hormone (levothyroxine [LT4]) (n=38); those with a history of thyroid cancer (n=14); those with missing covariates (n=8); and those with overt hyperthyroidism (TSH level of <0.10 mIU/L with elevated fT4 level) owing to the small patient number (n=1). There were no pregnant individuals. The final study population included 1,060 individuals.
2. Assessment of Thyroid Status
The serum TSH, fT4, and TPO Ab levels were measured using electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany) according to the criteria of the College of American Pathologists. In the main analysis, the Korean reference interval for the serum TSH level (0.62–6.68 mIU/L) was used, which is higher than that of Western countries [2]. This reference range reflects the 2.5th and 97.5th percentile of the serum TSH levels of the reference population, defined as the population with no history of thyroid disease or thyroid cancer and no history of taking medications that could influence thyroid function, with no family history of thyroid disease, with negative TPO Ab findings, and with serum fT4 levels within the reference range (0.89– 1.76 ng/mL), as previously reported; this population did not include pregnant women [2]. In the supplemental analysis, thyroid status was classified using the manual TSH reference range from Roche Diagnostics (0.35–5.50 mIU/L). The manual reference range for the serum fT4 level (0.89–1.76 ng/mL) was used in both main and supplemental analyses. The reference range for the TPO Ab level was <34 IU/mL.
3. Classification by Thyroid Status
As described in a previous study, the subjects were classified into the following groups according to their thyroid function test results [13]. Using the population-based TSH reference range (0.62–6.68 mIU/L), thyroid status was classified as follows: overt hypothyroidism was defined as a TSH level of 20 mIU/L or more or a TSH level of more than 6.68 mIU/L with an fT4 level below normal (<0.89 ng/mL) (n=10); subclinical hypothyroidism was defined as a TSH level of more than 6.68 mIU/L and less than 20 mIU/L with a normal fT4 level (0.89–1.76 ng/mL) (n=31); euthyroid was defined as a normal TSH level (0.62–6.68 mIU/L) (n=987); subclinical hyperthyroidism was defined as a TSH level of 0.10–0.6199 mIU/L or less than 0.10 mIU/L with a normal fT4 level (n=32); and overt hyperthyroidism was defined as a TSH level of less than 0.10 mIU/L with an elevated fT4 level (n=1). The subject with overt hyperthyroidism (n=1) was excluded owing to the small patient number. In the supplemental analysis, thyroid status was classified in a similar manner using the manual TSH reference range from Roche Diagnostics (0.35–5.50 mIU/L).
4. Assessment of the EuroQol-5 Dimension Three-Level Version Utility Values
Health-related quality of life was assessed using the EQ-5D-3L, a generic preference-based measure consisting of five questions concerning the current health status of patients [14]. The questions target five areas: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each question has three possible responses, i.e., no problem, some problems, or severe problems. Population-specific value sets used for deriving utility values from responses to questions enable effective comparison across different populations. The EQ-5D-3L has been widely used as a standard measure of health-related quality of life. The Korean EQ-5D-3L was developed by the Korea Centers for Disease Control and Prevention according to procedures outlined by the EuroQol group. The utility values for the Korean EQ-5D-3L range continuously from -0.171 (worst health status) to 1.000 (best health status).
5. Key Variables and Statistical Analysis
The considered covariates included age (years; continuous), sex (male or female; categorical), body mass index (kg/m2; continuous), household income (lower half or upper half; categorical), education (≤6 years or >6 years; categorical), employment status (unemployed or employed; categorical), smoking status (nonsmoker or current and past smoker; categorical), drinking status (nondrinker or drinker; categorical), physical activity (meets or does not meet requirements; categorical), diabetes (with or without; categorical), hypertension (with or without; categorical), dyslipidemia (with or without; categorical), serum hemoglobin level (mg/dL; continuous), and serum TPO Ab level (normal or high; categorical). Physical activity was calculated as metabolic equivalent task (MET) minutes per week using the International Physical Activity Questionnaire in 2013 and Global Physical Activity Questionnaire in 2014 and 2015 [15,16]. It was classified as not meeting the requirements (<600 MET-min/wk) or meeting the requirements (≥600 MET-min/wk). Further, the TPO Ab levels were classified into normal (≤34 IU/mL) or high (>34 IU/mL).
The chi-square test was used for categorical variables and one-way analysis of variance for continuous variables to test for significant differences in the means across the different thyroid status groups. Subsequently, an adjusted linear regression analysis was performed to test for significant differences in the EQ-5D-3L values across the sample groups (Table 2). Ninety-five percent confidence intervals were applied, and P-values of <0.05 were considered statistically significant for all results. All statistical analysis was performed using STATA ver. 14.0 (STATA Corp., College Station, TX, USA).
6. Ethics Statement
Prior to the survey, all participants of the sixth KNHANES provided informed consent. As the national survey data used for this study were publicly available from the Korea Centers for Disease Control and Prevention, no ethical approval from our Institutional Review Board was necessary.
RESULTS
1. Characteristics of the Study Population
The study subjects were a disease-free population (n=1,060) whose baseline characteristics are shown in Table 1. Their mean age was 65.4 years, and the proportion of men was 51.1%. There were 10 subjects in the overt hypothyroid group, 31 subjects in the subclinical hypothyroid group, 987 individuals in the euthyroid group, and 32 subjects in the subclinical hyperthyroid group (Table 1). Significant differences in the means were observed across the groups only for smoking status, physical activity, and hemoglobin levels (P=0.034, 0.033, 0.011, respectively). Across the sample groups, the overt hypothyroid group demonstrated the highest unadjusted mean EQ-5D-3L utility value, although the association was not significant (0.9497, P=0.599).
2. Adjusted Mean EuroQol-5 Dimension Three-Level Version Utility Values according to Thyroid Status
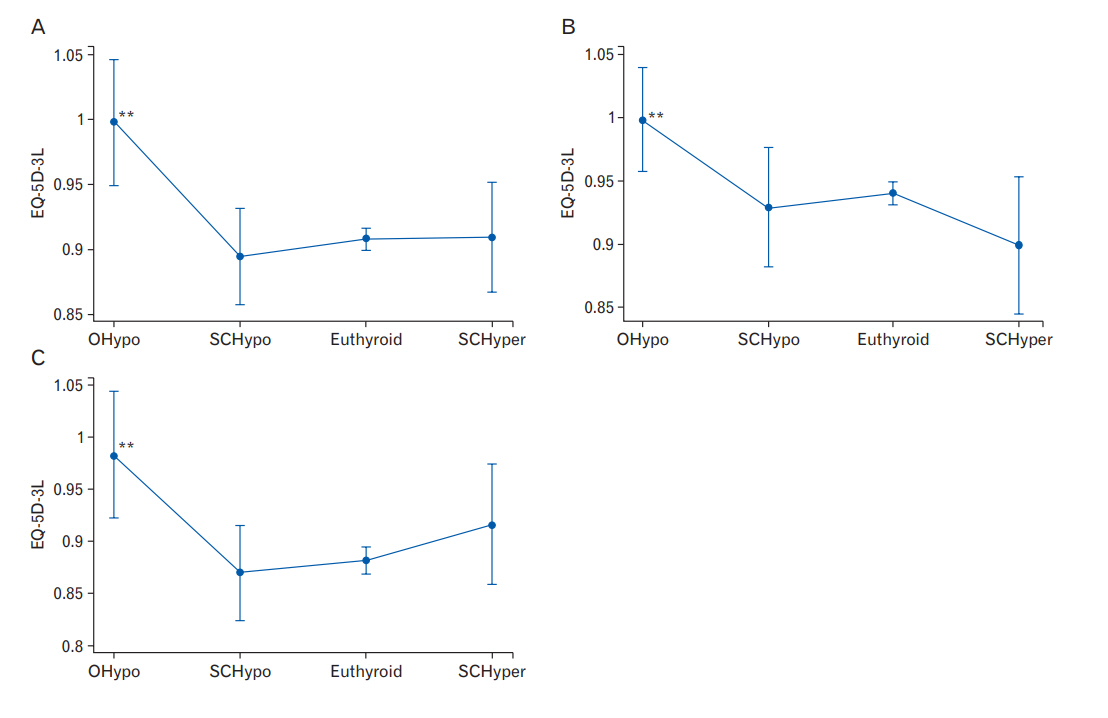
In the adjusted analysis, the overt hypothyroidism group had significantly higher mean least-square EQ-5D-3L utility values than the euthyroid group in the total population as well as in the male and female subpopulations (0.998 versus 0.908, 0.998 versus 0.940, 0.983 versus 0.882; P=0.000, 0.008, 0.001, respectively) (Table 2). At baseline of euthyroid, neither the subclinical hypothyroid group nor the subclinical hyperthyroid group showed a significant association (Table 2, Figure 1).
3. Categorization based on Population-Specific (0.62–6.68 mIU/L) versus Manual-Based Thyroid Stimulating Hormone Reference Ranges (0.35–5.50 mIU/L)
When thyroid status was classified using the manual-based TSH reference range (0.35–5.50 mIU/L) instead of the population-based TSH reference range (0.62–6.68 mIU/L), the distribution of individuals in each group shifted slightly (Supplementary Table 1). There were 11 subjects in the overt hypothyroid group, 61 subjects in the subclinical hypothyroid group, 977 subjects in the euthyroid group, and 11 subjects in the subclinical hyperthyroid group (Supplementary Table 1). Significant differences were observed across the groups only for smoking, drinking and hemoglobin levels (Supplementary Table 1). The unadjusted mean EQ-5D-3L utility values were the highest in the overt hypothyroid group, although the association was not significant (P=0.714) (Supplementary Table 1). In the adjusted analysis, the mean least-square EQ-5D-3L utility values increased in the overt hypothyroid group relative to the euthyroid group, although the association was not significant (0.968 versus 0.908, P=0.106) (Supplementary Table 2, Supplementary Figure 1).
DISCUSSION
In this nationwide, population-based, cross-sectional study using the sixth KNHANES data, we showed that a significant association might exist between overt hypothyroidism and higher EQ-5D-3L utility values in Korean subjects aged over 60 years (Table 2). This result suggests that asymptomatic older adults with TSH and fT4 levels that correspond to overt hypothyroidism might have better health-related quality of life than their euthyroid counterparts.
Several previous studies have reported on the relationship between hypothyroidism and measures of health-related quality of life in older adults, including mobility, self-care, usual activity, pain/disability, and anxiety/depression. For instance, a prospective population-based study conducted in participants followed up from age 85 to 89 years showed that increasing levels of TSH at baseline were associated with significant decelerated increases in disability in instrumental activities of daily living [6]. Another prospective population-based study of healthy asymptomatic older adults aged 70 to 79 years showed that their mild subclinical hypothyroid group demonstrated better mobility and had a higher percentage of those with good cardiorespiratory fitness and who reported walking in ease than did their euthyroid group [3]. Finally, a study using data from the Korean Longitudinal Study on Health and Aging on Korean subjects aged over 65 years found that subclinical hypothyroidism was not associated with cognitive impairment, depression, or poor quality of life in the elderly [11]. Some of these studies differ from our study in that the study population consisted of patients with subclinical hypothyroidism, rather than those with overt hypothyroidism. Moreover, these studies differed from our study in terms of the age of the study population.
Several mechanisms can possibly explain our finding that older adults aged over 60 years with overt hypothyroidism have better health-related quality of life than their euthyroid counterparts. Thyroid hormone plays a critical role in energy metabolism. Overt hypothyroidism may slow the metabolic rate, which may result in increased preservation of physical and cognitive functions [6]. This protective effect of overt hypothyroidism has been reported in the oldest old aged at least 70 years [5]. In young and middle-aged humans, the negative effects of hypothyroidism, such as dyslipidemia and adverse cardiovascular outcomes, are more dominant [5].
Clinical practices concerning the treatment of hypothyroidism in the elderly are mostly similar in the United States and in Korea. Screening for hypothyroidism is performed by measuring the serum TSH level [17,18]. Treatment with LT4 is recommended for symptomatic older adults with persistently elevated TSH levels and decreased fT4 levels [18,19]. The dose of LT4 depends on such factors as the presence and severity of thyroid-related symptoms and coexisting diseases, e.g., coronary artery disease and heart failure [18,19]. Older adults without risks of heart diseases may be initiated on a full dose of LT4 (1.6 mcg/kg/d), while those with risks are started on a lower dose (25–50 mcg/d) that is increased gradually [18,19]. For subclinical hypothyroidism, treatment remains controversial, as no benefit was observed with treating patients aged over 70 years [17,18,20-23].
While the target TSH reference range is 0.5–4.5 mIU/L for the general population, it is recommended that the target serum TSH level be set to approximately 4–6 mIU/L in individuals aged over 70 years, as the TSH levels tend to increase in older adults even without thyroid disease [17,18]. It is important to determine the optimal TSH target levels, as the elderly are especially susceptible to the adverse effects of excess LT4, such as atrial fibrillation and osteoporotic fractures [18]. In both the United States and Korea, there is a lack of randomized controlled studies of LT4 treatment in elderly patients with hypothyroidism comparing different TSH target values [18,19]. By showing that healthy asymptomatic Korean older adults without evident thyroid disease experience better quality of life at elevated TSH levels, our study highlights the importance of determining population-specific TSH target values for LT4 treatment in older adults.
Our study is the first to utilize data from the sixth KNHANES to investigate the association between thyroid status and health-related quality of life. One strength of our study is that as our results were derived from a large and reliable national dataset, they are more likely to be representative of the findings of the general population. Furthermore, we used both population-specific and manual-based reference ranges for TSH in our analyses. It has been reported that TSH levels vary across different geographic and ethnic groups [2]. According to a previous KNHANES study, the Korean reference population demonstrates higher TSH levels than does the US population, which is most likely attributed to the fact that Korea is an iodine-sufficient region [1,2]. Our study demonstrates that the association between overt hypothyroidism and EQ-5D-3L values is maintained even when the manualbased TSH reference range is used, although the statistical significance is lost (Supplementary Table 2).
One limitation of our study is that as it is based on cross-sectional data, we only observed TSH levels measured on a single occasion. For the same reason, we could not follow up on participants to investigate the effect of thyroid status on long-term outcomes or determine cause and effect. Further, owing to the small sample size of the overt hypothyroid group, which accounted for less than 1% of the total study population, our results, while statistically significant, are not sufficient to make any definitive statements and need to be substantiated by further research. As we performed our analyses based on data from the Korean population, it is unknown whether our conclusions will apply to other racial populations. Lastly, we were not able to measure the components of EQ-5D-3L, such as physical performance, directly.
In conclusion, our study suggests that overt hypothyroidism in older adults might be significantly associated with improved health-related quality of life. Moreover, several previous studies have reported that asymptomatic older adults with thyroid function test findings corresponding to overt or subclinical hypothyroidism tend to have better physical function and comparable rates of depression and cognitive impairment relative to their euthyroid counterparts. Thus, further studies should be conducted to investigate the possible protective health effect of hypothyroidism in older adults.