Increasing Individual Target Glucose Levels to Prevent Hypoglycemia in Patients with Diabetes
Article information

Abstract
Hypoglycemia is one of the severe complications of diabetes. To prevent hypoglycemia, an emphasis is placed on maintaining an appropriate balance between nutrition, activity, and treatment, which can be achieved by the repetition of self-trials based on self-monitoring. Clinicians routinely focus on patients’ contribution, including timely intake of an adequate amount of carbohydrates, physical activity, antidiabetic medication, and abstinence from alcohol. Recently, many guidelines have highlighted the importance of clinicians’ factors and recommend individualized treatments according to lifestyle patterns and specific needs following the de-intensification of treatment. The optimal value of hemoglobin A1c (HbA1c) levels for blood glucose level regulation remains controversial among countries, but it generally does not exceed 8.0%. In populations that are at a risk of hypoglycemia, such as the older adults, it is advisable to adjust the target blood glucose level to less than 8.0%. Meanwhile, a blood glucose level of 7.0%–7.5% is generally recommended for healthy older adults. If the expected lifetime is shorter than 10 years or in patients with chronic kidney disease and severe cardiovascular disease, the HbA1c level target can be increased to 7.5%–8.0%. For even shorter lifetime expectancy, the target can be adjusted up to 8.0%–9.0%. To prevent hypoglycemia, the target blood glucose level needs to be adjusted, particularly in older adult patients. Ultimately, it is important to identify the maximum blood glucose levels that do not cause hypoglycemia and the minimum blood glucose levels that do not cause hyperglycemia-associated complications.
INTRODUCTION
The Korean Diabetes Association (KDA) recommends an hemoglobin A1c (HbA1c) level of <6.5% as the general goal of blood glucose level management [1-8]. Most guidelines, such as those of the American Diabetes Association (ADA) [9-14], American Association of Clinical Endocrinologists (AACE) [15], European Association for the Study of Diabetes (EASD) [16], and International Diabetes Federation (IDF) [17,18], recommend an HbA1c level of <7.0% based on the stipulation that lowering the HbA1c level to its normal range reduces the risk of diabetes mellitus (DM)-associated complications. Some doctors often perceive this value as an absolute target for hyperglycemic control, but it is not. In certain conditions, lowering the HbA1c level to a general target level would do more harm than good. Various studies reported an increased risk of hypoglycemia, weight gain, and cardiovascular disease from active treatment [19-21]. Strict blood glucose level management in the early stages of diabetes helps to reduce the incidence of complications. However, for patients with longer periods of diabetes who already developed cardiovascular disease, active intensive blood glucose level management considerably increases the risk of hypoglycemia, cardiovascular disease, and mortality, rather than prevent complications. Therefore, the ADA, AACE, EASD, IDF, Japan Diabetes Society (JDS), and KDA have developed various strategies to prevent hypoglycemia [9-18,22-24]. Grossly, it is important to eat a well-balanced diet, perform regular exercise, and take appropriate medication to prevent hypoglycemia. In addition, individualized target goal is recommended according to lifestyle patterns and specific needs.
EDUCATION
Nothing is better than prevention, and most hypoglycemic events are preventable. For that, it is important to educate both patients and their family, who should be informed about the possible causes of hypoglycemia and preventive strategies, regarding the risk of hypoglycemia. Previous studies suggest that the common causes are dietary factors, excessive physical activity, stress, and medication misadventures [25]. It is necessary to determine the effect of carbohydrate intake, physical activity, and use of antidiabetic medications on blood glucose level. A comprehensive strategy for proper balance of nutrition, activity, and medication is needed to prevent hypoglycemia. Although newer antidiabetic medications are less dependent on mealtime, moderate amount of carbohydrate intake on regular mealtime is generally an important nutritional management for diabetic patients. Carbohydrate counting is useful especially for patients receiving rapid-acting insulin treatment. This technique may require the adjustment of food intake and/or antidiabetic medications before performing physical activities or sleeping to prevent hypoglycemia. Appropriate balance between nutrition, activity, and treatment can be achieved by repetition of selftrials based on self-monitoring.
Patients should pay attention to nocturnal hypoglycemia as more than 50% of cases of severe hypoglycemia occur at night [26]. Regardless of whether or not blood glucose levels are well controlled, patients should consult their doctors if nocturnal hypoglycemia occurs frequently. The target blood glucose levels for those with or without nocturnal hypoglycemia are yet to be established. Regular consumption of snacks to prevent nocturnal hypoglycemia in patients with type 1 DM is not recommended [27]. In patients who take medications for diabetes control twice daily, severe hypoglycemia can occur at dawn if they eat dinner early or consume insufficient protein at dinner; thus, taking snacks before bedtime is recommended. Patients with blood glucose levels of 100–140 mg/dL are advised to measure their blood glucose levels before bedtime. Those with lower blood glucose levels (<100 mg/dL) before bedtime are recommended to eat snacks containing glucose and protein (e.g., one glass of milk and half a banana) before bedtime [28].
Blood glucose level regulation also remains important in patients with a history of chronic alcohol consumption or those who are intermittent heavy drinkers [29]. Alcohol intake is absorbed in the stomach and intestines, which can interfere with the metabolism of other nutrients and cause hypoglycemia by blocking gluconeogenesis. Drinking alcohol on an empty stomach or immediately after exercise can cause hypoglycemia. Patients with diabetes are advised to abstain from drinking alcohol, but those who cannot are recommended to only drink alcohol once or twice weekly after meals and only 1 or 2 glasses at a time [30]. The recommendations for alcohol consumption to reduce the risk of hypoglycemia related to alcohol drinking in those with diabetes are shown in Table 1 [31].

INDIVIDUALIZED GLUCOSE TARGET
There is no rationale to deliberately avoid active blood glucose level management in patients without severe cardiovascular disease or those with risk of hypoglycemia or other adverse conditions. If it is safe and appropriate to use oral hypoglycemic agents (OHA) or insulin, targeting an HbA1c level of <6.5% of would help prevent microvascular and macrovascular complications. In contrast, in patients with advanced age, history of severe hypoglycemia, short life expectancy, renal disease, macrovascular complications, severe illnesses, or type 2 DM who cannot achieve an HbA1c level of <6.5% without intensive care, it is reasonable to increase the blood glucose level target and to provide a safe line to use the reduced doses of OHA or insulin without overtreatment. In particular, if there are no hyperglycemia symptoms, such as polyphagia, polydipsia, or polyuria, it is reasonable to increase the HbA1c level target. If the life expectancy is shorter than 10 years, the HbA1c level target could be 7.5%–8.0%. If there are comorbidities such as cognitive disorder, chronic kidney disease, and severe cardiovascular disease, an HbA1c level of ≤8.0% is recommended. The JDS also states that although the general target for HbA1c level is <7.0%, treatment targets should be individualized to <8.0% if there is a risk for hypoglycemia [22-24]. The American College of Physicians stated that the standard HbA1c level of <7.0% recommended by the Institute for Clinical Systems Improvement increases the risk of death, weight gain, hypoglycemia, and other adverse events and does not reduce the mortality rate [32]. Despite the differences in the recommended levels, the common recommendation of professional diabetes societies is that the optimal HbA1c level goal should be increased in patients with high risk of hypoglycemia.
Older adult patients with diabetes are at an increased risk of hypoglycemia because they are more vulnerable to malnutrition due to anorexia, experience difficulty in masticating or swallowing, and have digestive disorders. Thus, it is important to monitor the risk of hypoglycemia due to insufficient food intake when caring for older patients with diabetes. In addition, physiological and cognitive functions, lifestyle patterns, and risks of hypoglycemia should be assessed in this population, and treatment goals should be individualized. Treatment goals are set to assess the effects of long-term blood glucose level management. If the patient is active and has no cognitive impairment, the goal of blood glucose level management can be similar to that of other young patients. However, if patients have advanced diabetes complications, a short life expectancy, or serious cognitive and functional disorders, blood glucose level control should be enforced less strictly. The American Geriatric Society recommends an HbA1c level of 7.5%–8.0% in the general patient population, 7.0%–7.5% in healthy patients, and 8.0%–9.0% in those with a short life expectancy [33]. Despite these varying targets, hyperglycemia that may cause diabetes symptoms or acute complications should be avoided in all cases. The IDF generally recommends that physicians should carefully monitor hypoglycemia in patients with a fasting blood glucose level of <110 mg/dL and an HbA1c level of <7% [17,18]. In such patients, the physician should prescribe drugs with a low risk of hypoglycemia. Moreover, all patients who take insulin or hypoglycemia-causing diabetic drugs should measure their blood glucose levels regularly, create emergency contacts, and develop a treatment plan for hypoglycemia. The JDS also recommended that in older patients, the lower limit of HbA1c level should be increased to 6.5%–7.5% depending on their cognitive function or their performance of daily living activities [22-24].
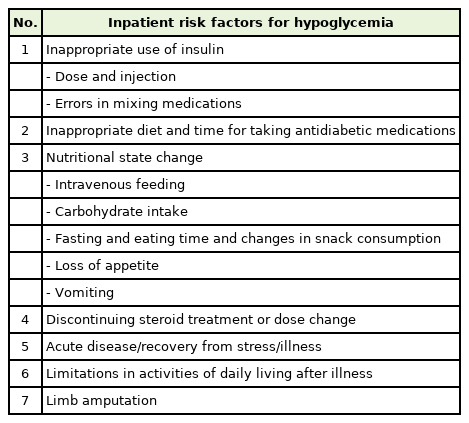
Blood glucose levels tend to be more strictly controlled in hospitalized patients or those with severe conditions, but glucose control can increase the risk of hypoglycemia [33]. Intensive blood glucose level management during hospitalization is routine clinical practice, but it increases the risk of death from hypoglycemia. Therefore, the blood glucose of inpatients is not targeted at 80–100 mg/dL. Moreover, the preprandial blood glucose level is generally set to <140 mg/dL, and the random blood glucose level is <180 mg/dL. For patients with severe underlying disease, the target blood glucose level is 140–180 mg/dL. If the life expectancy is shorter or the patient has terminal disease, the blood glucose level control target should be enforced less strictly (Table 2) [34].
SELECTION OF TREATMENT
A more effective and simple way to prevent hypoglycemia is to reconsider antidiabetic medications [35]. Though the harm of intensive treatment would exceed the benefits for those with high risk of hypoglycemia, most of them were treated with insulin or sulfonylureas, which are the most common medication causing hypoglycemia [36]. The selection of medications should be based on the overall patient condition, including audiovisual disorders, malnutrition, muscle loss, cognitive and emotional functions, physical functions, and concomitant treatment. Older adults or patients with advanced renal or hepatic diseases and dementia are prone to hypoglycemia due to poor kidney or liver function, irregular meal consumption, and drug interactions from multidrug treatment. Hence, it is reasonable to de-intensify antidiabetic treatment, simplify treatment regimens, or use other medications with relatively low risk of hypoglycemia. Moreover, insulin and OHA should be started at low doses and gradually increased.
CONCLUSION
The ADA, AACE, EASD, IDF, JDA, and KDA have developed various strategies to prevent hypoglycemia, including increasing the target blood glucose level in patients with high risk of hypoglycemia [9-18,22-24]. Strategies focus not only on patients’ factors such as moderate meal intake, consumption of snacks during exercise and before bedtime to prevent hypoglycemia, and abstinence from alcohol but also clinicians’ factor such as individualized treatment goal and prescription according to lifestyle patterns and specific needs. Most members of the diabetes healthcare team are only aware of the general goals of blood glucose level management and are often unfamiliar with the adjustment of blood glucose level targets. In clinical practice, blood glucose level targets are often increased based on experience rather than any systematic basis [37]. Clinicians should identify the maximum level of blood glucose level that will not cause hypoglycemia-related complications. Our future studies are aimed at developing a systematic basis for such adjustments.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by a grant from the Korea Institute of Drug Safety and Risk Management in 2018.