Age-Related Difference in Weight Change and All-Cause Mortality in Middle-Aged and Older Korean Populations: Korean Longitudinal Study of Aging
Article information

Abstract
Background
Obesity is associated with increased mortality as a significant risk factor for chronic diseases, including cardiovascular diseases and cancer. Several people believe that weight gain is harmful, and weight loss helps maintain health. However, some studies have shown that weight loss, particularly among older adults, is more likely to increase the risk of mortality than weight gain.
Methods
We used data for the cohort of the Korean Longitudinal Study of Aging, which is a nationwide stratified multi-stage sample of adults aged 45 years. The all-cause mortality risk was assessed using the survival status and the number of months of survival calculated from 2006 (baseline year) to 2016. Cox proportional hazard regression were used to study the causal link between weight change and all-cause mortality risk.
Results
The results showed interactive associations between weight loss and mortality among middle-aged and older adults. The hazard ratio was 1.62 (95% confidence interval [CI], 1.10–2.40) for the participants aged 45–65 years with weight losses greater than 5 kg and 1.56 (95% CI, 1.29–1.89) for those older than 65 years with weight losses greater than 5 kg. The results for the group with weight gain above 5 kg were not significant. Middle-aged and older men showed an increase in all-cause mortality associated with weight loss of more than 5 kg, but only the older women showed significant results.
Conclusion
This large-scale cohort study in Korea showed a relationship between weight loss and all-cause mortality in middle-aged and older individuals.
INTRODUCTION
A significant change in weight can cause various health problems and may also affect all-cause mortality [1,2]. In general, weight gain is harmful, and weight loss is beneficial for health. Obesity is an important contributor to the increase in mortality rate as a major cause of chronic diseases, including type 2 diabetes mellitus, hypertension, cardiovascular diseases (CVDs), and some cancers [3,4]. However, the results of previous studies on the association between weight change and mortality are rather inconsistent, based on other population conditions or study groups. Some studies have shown that weight loss is associated with an increase in mortality [5-8]. Andres et al. [5] reviewed 13 studies on the association between weight change and all-cause mortality, concluding that some degree of weight gain during adulthood lowers allcause mortality while weight loss is associated with an increase in allcause mortality. A previous study reported the association between weight change and mortality in older adults in Norway after 14 years of follow-up, concluding that minimal weight loss of ≥5% or >3 kg was significantly associated with an increased risk of mortality in people older than 71 years [7]. However, some studies have found that extreme weight changes, both gains and losses, within a year are not strongly associated with mortality [9]. For example, a study of older Mexican Americans found that weight gain led to a decrease in mortality [10].
The results of several studies on weight change and mortality tend to differ with age. The reports of the effects of weight changes from early to late adulthood or mid to late adulthood on mortality risk are not entirely consistent [6,11-14]. A recent prospective cohort study of the US population pointed out that weight gain from early to mid-adulthood was associated with an increased risk of all-cause mortality. Weight loss during this period was not significantly related to mortality, while the association between weight loss from mid to late adulthood has become stronger and more significant [15]. As such, the significance of the weight change can differ with age. With the continual aging of society, it is necessary to demonstrate the correlation between the change in weight and the mortality rate through community research. We conducted this study to investigate the association between weight change and all-cause mortality using the data of the cohort of the Korean Longitudinal Study of Aging (KLoSA), which is a nationwide stratified multistage sample of adults.
METHODS
1. Study Population
We used data from the 10-year (2006–2016) cohort of the KLoSA, which is a nationwide stratified multistage sample of adults aged 45–79 years. The all-cause mortality risk was evaluated using the survival status (death, dropped out, or survival) and months of survival (personmonths) calculated from 2006 (baseline year) to 2016. The study initially included 10,254 individuals, and we excluded 2,194 individuals who had missing health information at baseline. Finally, 8,060 individuals were included in the study. Information on the day of death and the cause of death was obtained from family members and death certificates. All participants of this study based on the KLoSA database provided written informed consent, and the survey protocol was approved by the Institutional Review Board of Statistics Korea. In addition, this study was approved by the Institutional Review Board of Daegu Catholic University Hospital (CR-20-074).
2. Main Exposure: Weight Change
The question of weight change was asked based on a baseline survey. In this study, the weight change in the cohort was based on the weight of the first survey (2006), and the difference from the weight of the second survey (2008) was calculated. The weight changes were categorized into three: loss or gain of less than 5 kg (‘stable’, considered the reference category), gain of 5 kg, and loss of 5 kg.
3. Covariates
The participants were interviewed on their demographic characteristics and health behaviors using a self-administered questionnaire. The demographic variables were age (45–65 years or ≥65 years), marital status (married or single), level of education (≤6 years, 7–11 years, 12– 15 years, or ≥16 years), and annual household income (<10,000,000 Korean won [KRW], 10,000,000–30,000,000 KRW, or >30,000,000 KRW). Cognitive function was assessed using the Korean version of the Mini-Mental State Examination (MMSE-K). To assess functional status, activities of daily living (ADL) and instrumental activities of daily living (IADL) were measured. Health behavior variables included cigarette smoking (current smoker, former smoker, or never smoked) and alcohol use (current drinker, former drinker, or non-drinker). In addition, the body mass index (BMI) was calculated using height and weight. The health status variable corresponds to the number of chronic diseases. The data were collected based on a history of self-reported diseases. Respondents reported the presence of one or more diseases diagnosed by the physician, including hypertension, diabetes mellitus, cancer, chronic lung disease, chronic liver disease, CVD, stroke, arthritis, and psychiatric disorders. The respondents were divided into groups (0, 1, and more than 2 [multimorbid]) based on the number of chronic conditions.
4. Outcome Assessment
The main outcome of this study was mortality from all causes. The mortality risk was assessed using survival status and months of survival calculated from 2006 (baseline) to 2016. The number of deaths over a maximum follow-up period of 10 years was determined using death certificates.
5. Statistical Analysis
To investigate the association between weight change and all-cause mortality, a statistical analysis was performed in two directions. First, Pearson’s chi-square test was used for the comparative analysis of the groups. Second, Cox proportional hazard regression was conducted longitudinally to investigate the association between weight change and mortality. The hazard ratios (HRs) for all-cause mortality with 95% confidence intervals were calculated. All the analyses were conducted using IBM SPSS ver. 19.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at P<0.05.
RESULTS
Table 1 shows the demographic characteristics of participants stratified by the weight change category. In the middle-aged group, 10.4% gained weight and 13.0% lost weight, compared with 12.0% and 17.3%, respectively, in the older adult group. Compared with the stable weight group, persons in the weight gain group had significant differences in variables such as BMI, MMSE, and alcohol consumption across all age groups. In the weight gain group, the middle-aged group was more likely to have lower household income, higher MMSE scores, and more current smokers and current drinkers. The older adult group was more likely to have lower education levels; higher ADL, IADL, and MMSE; and fewer current drinkers. The weight loss group had a higher mean BMI and was more likely to have lower household income and higher ADL, IADL, and MMSE scores at all ages. The middle-aged group was more likely to have multimorbidity, while the older adult group was more likely to have a single marital status and lower levels of education.

General characteristics of participants by age group
Table 2 presents the multivariate-adjusted HRs for the cause of all deaths by comparing the respondents with a reference group of people with weight changes of less than 5 kg. The HRs for weight loss were 1.59 (95% CI, 1.34–1.89) for all ages and 1.62 (95% CI, 1.10–2.40) for middle-aged and 1.56 (95% CI, 1.29–1.89) for older adults. No significant association between weight gain and all-cause mortality was observed among the groups.

Multivariable-adjusted HRs for all-cause mortality of individuals with weight change from baseline (2006)
The subgroup analysis revealed different outcomes between men and women. The HRs for all-cause mortality based on the results of the multivariable model for the middle-aged and older adults were 1.94 (95% CI, 1.20–3.12) and 1.60 (95% CI, 1.23–2.08) for men with weight loss of more than 5 kg, respectively. Among older women, the HR for weight loss of more than 5 kg was 1.56 (95% CI, 1.17–2.08). There were no significant differences between the men and women in the weight gain group (Table 3).
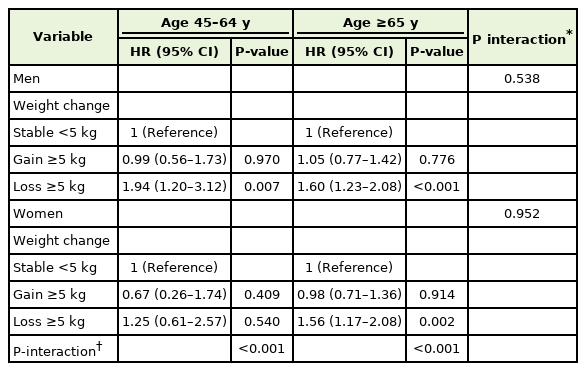
Sex-specific multivariable HRs for all-cause mortality with individuals with weight change of middle-aged and older adult
DISCUSSION
Our study of 8,060 adults aged 45–79 years at baseline showed that a weight loss of more than 5 kg over the previous 2 years was associated with a higher risk of all-cause mortality over the next 10 years of follow-up. This was observed after adjustment for covariates, age, sex, household income, educational level, ADL, IADL, MMSE, BMI, multimorbidity, smoking, and alcohol intake. In men, there was an increase in all-cause mortality with a weight loss of more than 5 kg in the middle-aged and older adult groups. In women, the result was only significant in the older adults. There were no significant differences in weight gain and all-cause mortality across all age groups.
This finding on the association between weight loss and mortality above middle age is consistent with previous studies [14,16-18]. Several studies have shown that weight change and all-cause mortality show a reverse J-shaped curve, indicating that the effect of weight loss was stronger than that of weight gain on mortality. In a nationwide study of Korean adults involving 11,524,763 participants, weight loss was associated with higher mortality rates than weight gain; the group with weight loss of ≥15% had the highest HR for all-cause mortality (HR, 2.598; 95% CI, 2.537–2.659). The HR for all-cause mortality in the group with weight gain of ≥20% was 1.784 (95% CI, 1,695–1.877) [19]. Another study showed that moderate to large weight gains and losses were risks for all-cause and CVD-related mortality in middle-aged and older individuals, with a slightly higher risk for weight loss than weight gain [20].
Some studies suggest that weight loss in middle-aged people predates a rise in mortality. In men aged 40–65 years, those who lost the most weight (>5 kg) experienced the highest rate of mortality, particularly from coronary heart disease and not from cancer, especially in lean persons [21]. The prospective cohort study of the US National Health and Nutrition Examination Survey reported that weight gain during adulthood and weight loss during middle adulthood were particularly associated with a high risk of death from heart disease [15]. In our study, the association of mortality with weight loss became stronger and significant during middle to late adulthood.
The mechanism underlying the association between weight loss and mortality is unclear, but changes in body composition, such as reduced muscle mass, especially in older adults, may be considered [22]. Weight loss in older adults is associated with frailty, which is correlated with morbidity, falls, disability, and hospitalizations [23], and weight loss is associated with oxidative damage of DNA [24] and may weaken the immune system [25], which increases the incidence of cancer and related mortality.
In our study, there was a statistically significant increase in all-cause mortality with a weight loss of more than 5 kg in older women. Considering the difference between sexes, women are known to have a much lower risk of mortality from CVDs than men before menopause. A prospective cohort study showed that men had higher CVD mortality than women across all categories of anthropometric measures of obesity, but this gender difference in CVD mortality somewhat diminished in obese individuals [26].
Similar to our study, certain studies have found inconclusive results on the association between weight gain and all-cause mortality. A study of 12,580 EPIC (European Prospective Investigation into Cancer)-Norfolk participants concluded that weight loss was associated with higher mortality, but weight gain outcomes were inconclusive over 15 years of follow-up [27]. However, one study reported an inverse association between weight gain and all-cause mortality in Japanese men. However, the association between weight gain and mortality is not clear for Japanese women [28]. Several community-based cohort studies on weight gain and mortality are inconsistent. Several studies have shown an association between weight gain and increased mortality [5,14]. However, some studies have reported no association between weight gain and mortality [2,9,10,29]. The controversial findings may result from the study design, age of the participant, and the observation period. In a US population study, the degree of weight gain was associated with mortality. A weight gain of 5%–15% was not associated with an increase in mortality, but a weight gain of more than 15% was associated with a decrease in mortality in underweight older adults [6]. The reason for the greater effect of weight loss on mortality than weight gain can be explained by the weight tolerance associated with aging [30]. Consequently, weight gain has an inverse effect on weight loss in relation to mortality.
This KLoSA study provides a large cohort of free-living, middle-aged, and older men and women with a prolonged follow-up and assesses the effects of numerous variables on health practices. However, this study has certain limitations. First, based on the data, we determined whether the weight change was intentional or not. Similarly, we could not determine whether the change in weight was due to changes in exercise habits or diet. Second, data collection was based on self-reporting, which is a common method in community-based epidemiologic studies, but there is the potential for inaccuracy and subjectivity. Data for the limited variables were collected using questionnaires about multiple factors that may have been involved in mortality risk.
This large-scale cohort study in Korea demonstrated a relationship between weight changes and all-cause mortality. Weight loss was significantly associated with an increase in all-cause mortality in the Korean middle-aged and older men and women, but showed no significant effect on weight gain and mortality regardless of age.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.