Association between Problematic Smartphone Use and Physical Activity among Adolescents: A Path Analysis Based on the 2020 Korea Youth Risk Behavior Web-Based Survey
Article information

Abstract
Background
Physical activity is known to prevent several diseases and positively affect mental health. Previous studies have shown that smartphone addiction negatively affects the physical activity of children and adolescents. This study aimed to investigate the relationship between problematic smartphone use and physical activity among adolescents and the related factors using path analysis.
Methods
Using data from the 16th Youth Risk Behavior Web-based Survey from 2020, scores on the Smartphone Addiction Scale—Short Version for Adolescents, physical activity, sex, socioeconomic status (SES), academic performance, depression, smoking, drinking, and sitting time were assessed. Complex sampling and path analyses were performed.
Results
Of the total 54,948 students, 25.5% were smartphone risk users, including potential and high-risk users. The direct path coefficients of each factor indicated that female sex (-0.14 for male), low SES (-0.062), high academic performance (0.056), low sitting time for studying purposes (-0.033), high sitting time for non-studying purposes (0.071), and depressive mood (0.130) were related to problematic smartphone use (all P<0.001). Each factor affected problematic smartphone use, and subsequently had a negative effect on the amount of physical activity, with a direct path coefficient of -0.115 (P<0.001).
Conclusion
In this study, we confirmed that problematic smartphone use among adolescents was negatively associated with performing an adequate amount of physical activity and that various factors, such as sex, SES, academic performance, and sitting time, directly and indirectly affected this relationship.
INTRODUCTION
Physical activity encompasses any movement of the body that engages skeletal muscles and leads to energy expenditure. Engaging in regular physical activity is known to prevent several diseases, such as cardiovascular diseases, type 2 diabetes, and hypertension. Moreover, it promotes cardiorespiratory and musculoskeletal fitness [1]. Particularly, physical activity in children and adolescents positively affects cognitive function, academic achievement, and memory [2]. Additionally, it plays a significant role in maintaining normal weight and lowering the risk of experiencing depressive mood [1]. In addition, long sitting times in children and adolescents are associated with poor cardiometabolic health and fitness [3,4]. Sitting time is associated with obesity [3,4] and mental health disorders, including depressive mood [5].
Smartphones have led to lifestyle changes by integrating various functions. South Korea has high Internet and smartphone ownership rates. According to the 2021 Korea Media Panel Survey, the nationwide smartphone ownership rate in Korea was 92.8%, and that among adolescents aged 10–19 years was approximately 95.9%. Smartphones have made our lives convenient as they allow for easy accessibility to the Internet and are portable, which allows people to carry smartphones with them all the time; they have several advantages along with numerous adverse effects for adolescents [6]. According to the 2021 Smartphone Overdependence Survey, the smartphone overdependence group comprises 24.2% of all participants.
Prior research has consistently indicated that individuals at high risk of smartphone addiction exhibit markedly lower average daily walking steps and calorie consumption, suggesting that smartphone addiction negatively affects the degree of physical activity [7,8]. Moreover, excessive smartphone use has been associated with reduced real-life interactions, academic performance decline [9], and leads to several issues, such as memory disorders, decreased attention, headache, and fatigue [10]. However, previous studies have limitations, including small sample sizes, inaccurate application of smartphone overdependence scales, and inadequate consideration of other relevant variables. Thus, this study was designed to identify the relationship between smartphone addiction and physical activity in Korean adolescents using a large cross-sectional sample, and conduct a path analysis of factors influencing engagement in physical activity.
METHODS
1. Study Participants
This cross-sectional study was based on the 16th Youth Health Behavior Survey data in 2020. The youth health behavior survey was an anonymous, self-administered online survey of students between the first grade of middle school and the third grade of high school, and was conducted by the Ministry of Health and Welfare and the Korea Disease Control and Prevention Agency to investigate health behaviors among adolescents in Korea. The target population of this survey was defined as enrolled students studying in middle and high schools across the country as of April 2020; data on 54,948 students were used for analysis by extracting the samples using stratified cluster sampling.
This study was approved by the Institutional Review Board of Hanyang University Hospital (IRB approval no., 2022-05-058). The requirement for informed consent from individual patients was omitted due to the retrospective nature of this study.
2. Measurement and Classification of Smartphone Addiction
Smartphone addiction was assessed using the Smartphone Addiction Scale—Short Version for Adolescents, which is used to measure smartphone overdependence. The scale comprises 10 questions based on failure to control the use of smartphones (three questions), salience (three questions), and problematic outcomes (four questions). The responses for each question were scored as 4 points for “strongly agree,” 3 points for “agree,” 2 for “disagree,” and 1 for “strongly disagree,” leading to a total of 40 points.
According to this scale, adolescents with a score of ≥23 points were classified as a potential risk group and those with ≥31 points as a high-risk group. The potential-risk group was defined as a state of decreased control over smartphone usage in which interpersonal conflicts or problems in daily life begin to occur. The high-risk group was defined as a state of uncontrolled smartphone usage in which interpersonal conflicts and problems in daily life or health problems occur in an extreme manner. We considered the potential risk and high-risk groups as risk users, and the remaining groups using smartphones in a controlled manner as general users.
3. Assessment of Physical Activity
The questionnaire on engagement in physical activities comprises three questions, which were regarding moderate- and vigorous-intensity physical activities and muscle strengthening exercises. Regarding moderate-intensity physical activity, the question “How many days did you engage in physical activity (regardless of the type) for 60 minutes every day in last 7 days to a degree where your heart beats increased compared with the normal or you ran out of breath?” comprised responses from “0 day(s) a week” to “7 days a week.” For high-intensity physical activity, the question “How many days did you engage in high-intensity physical activity for >20 minutes every day in last 7 days to a degree where you ran out of breath or your body sweated? (high-intensity physical activities: jogging, soccer, basketball, Taekwondo, hiking, cycling at high speed, fast swimming, carrying heavy stuff, among others)” comprised responses from “0 day(s) a week” to “≥5 days a week.” For muscle strengthening exercise, the question “How many days did you engage in exercises in last 7 days to increase muscular strength by performing muscle strengthening exercises, such as push-up, sit-up, weightlifting, dumbbell workout, pull-up bar workout, and parallel bar workout?” comprised responses from “0 day(s) a week” to “≥5 days a week.” If moderate-intensity exercises were performed for ≥60 minutes every day and muscle strengthening exercises were performed ≥3 days a week, the participant was considered to have “practiced the physical activity guidelines.”
4. Other Measures
Other additional variables, including sex, socioeconomic status (SES), academic performance, depressive mood, current cigarette smoking, current alcohol consumption, total sitting time for studying in a week (min/wk), and total sitting time for non-studying purposes in a week (min/wk), were considered. The factors of SES and academic performance were categorized into “high,” “middle,” and “low” and were rated by the students themselves; moreover, experiencing depressive mood was answered as “yes,” or “no,” depending on whether they experienced depressive mood in past 12 months. The questionnaire on sitting times was structured in such a manner that the responses were in the unit of minutes, including “sitting time spent for the purpose of studying in last 7 days,” “sitting time for the purpose of studying during the weekend in last 7 days,” “sitting time spent for non-studying purposes in last 7 days,” and “sitting time spent for non-studying purposes during the weekend.” For analysis, these were further classified into “sitting time spent for the purpose of studying in the last week (min/wk)” and “sitting time spent for non-studying purposes in the last week (min/wk).”
5. Statistical Analysis
In this study, a cross-sectional analysis was performed as a complex sample analysis using IBM SPSS Statistics ver. 26.0 (IBM Corp., Armonk, NY, USA), and a path analysis was performed to investigate a possible causal relationship between the variables in the study model. Statistical analysis was performed using LISREL ver. 8.52 software (Scientific Software International Inc., Lincolnwood, IL, USA). For suitability of the model, suitability indices including root mean square error of approximation (RMSEA), goodness of fit index (GFI), comparative fit index (CFI), and normed fit index (NFI), which were not sensitively affected by sample sizes, were used rather than entirely relying on chisquare (χ2) values, which are sensitive to sample sizes. When RMSEA is ≤0.10 and CFI, GFI, and NFI values are ≥0.90, it is interpreted as a reasonable suitability.
RESULTS
1. General Characteristics
The general characteristics of the study participants according to smartphone risk are presented in Table 1. Of 54,948 students, 25.5% were addicted to smartphones. Approximately 21.2% of male and 30.0% of female students were smartphone risk users, indicating a higher risk among female students (P<0.001). In addition, 30.2% of the students were smartphone risk users with low SES, which was higher than the proportion of other students (25.0%). Moreover, 34.2% and 32.8% of students were smartphone risk users with current smoking and drinking habits, respectively, and had higher risks than non-smoking and non-drinking students (25.0% and 24.6%, respectively; P<0.001). Overall, 35.9% of the at-risk students experienced depressive mood in the past 12 months, showing higher risks than those who did not (21.9%) (P<0.001). Sitting time for the purpose of studying was 611.55 min/wk among risk users, and was lower than that among general users (634.47 min/wk), whereas sitting time for non-studying purposes was higher among risk users than among general users (591.48 min/wk versus 538.21 min/wk).

General characteristics of study participants (N=54,948)
2. Path Analysis
According to path analysis, all 18 paths for the total number of days of physical activity were statistically significant (Figure 1). It was found that problematic smartphone use directly affected the total number of days of physical activity, whereas SES affected the total number of days of physical activity via problematic smartphone use. Furthermore, it was found that sex, academic performance, sitting time for the purpose of studying, sitting time for non-studying purposes, current cigarette smoking, current alcohol consumption, and experiencing a depressive mood affected the number of days of physical activity directly or indirectly via problematic smartphone use. The direct path coefficients of male sex, SES, academic performance, sitting time for studying purposes, sitting time for non-studying purposes, and experiencing depressive mood on problematic smartphone use were 0.140, 0.062, 0.056, 0.033, 0.071, and 0.130, respectively. This indicates that female sex, low SES, high academic performance, short sitting time for studying purposes, long sitting time for non-studying purposes, and depressed mood are directly associated with problematic smartphone use. Each factor affected problematic smartphone use, which in turn negatively affected the number of days of physical activity, with a path coefficient of -0.115 (P<0.001).

Results of the path analysis. Path analysis model of sex, smoking, alcohol drinking, sitting time for studying and nonstudying purposes, socioeconomic status, academic performance, depressive mood, smartphone risk user, and physical activity. *P<0.01. **P<0.001.
A path analysis of the effect of problematic smartphone on the total number of days of physical activity via sitting time was conducted. The results showed that all four paths were significant (Figure 2). Problematic smartphone use negatively affected sitting time for studying purposes, whereas it positively affected sitting time for non-studying purposes, resulting in negative effects on the total number of days of physical activity as sitting time increased (P<0.001).
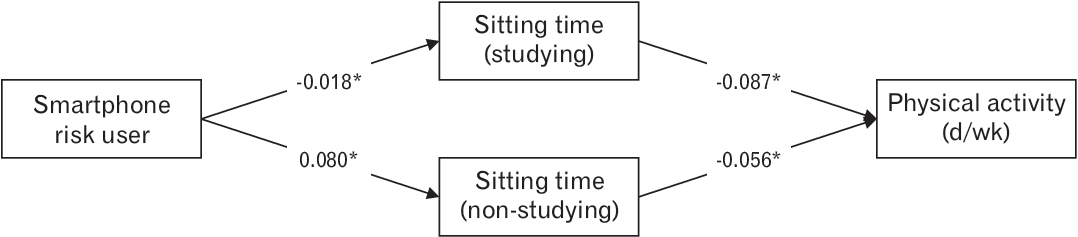
Path analysis of sitting time for studying and non-studying purposes, smartphone risk user, and physical activity. *P<0.001.
The results of suitability testing for each path model are listed in Table 2. The results revealed that each path was suitable.
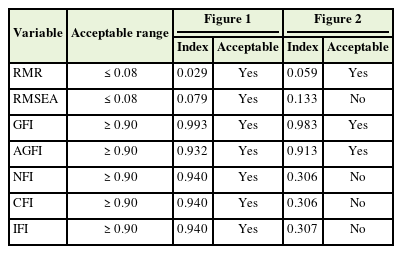
Goodness of fit indices for the model
DISCUSSION
This study revealed inadequate physical activity among Korean adolescents. Only 4.8% of the students followed the World Health Organization guidelines for physical activity, which is markedly low compared to the 19% of adolescents who, as of 2016, followed the physical activity guidelines worldwide. In the path analysis, smartphone risk users showed low levels of physical activity. Female sex, low academic performance, low SES, current smoking and drinking, and depressive mood were associated with a high risk of smartphone use, and these factors directly and indirectly affected low physical activity. In particular, longer sitting times for studying or non-studying purposes negatively affect physical activity.
The results of a previous study conducted on American college students were similar to those of our study, which reported that women spent more time on smartphones than men in a day sending text messages and emails and using social media sites most of the time [11]. Another study reported that individuals with younger age, depression, and extroverted personalities showed higher scores regarding the problematic use of smartphones [12]. A study on Korean adolescents found that the smartphone addiction group exhibited significant symptoms, such as depression, anxiety, and attention deficit hyperactivity disorder, compared to the normal group, and had a higher tendency for smoking and drinking [13]. Additionally, one study reported that a lower educational level was associated with a higher risk of smartphone addiction [14].
It can be inferred from this study that factors including sex, low SES, current smoking and drinking status, depressive mood, and high sitting time are associated with the risk of smartphone use and a subsequent decline in physical activity, which can negatively affect physical health. According to the results of another study conducted among American college students, the use of mobile phones interferes with physical activity during leisure time and promotes sitting, thereby decreasing cardiopulmonary health via maximal oxygen consumption [15].
Path analysis confirmed that female sex, low SES, low academic performance, and high sitting time increased the risk of problematic smartphone use, which in turn reduced physical activity. Among these factors, sitting time (either for studying or non-studying purposes) is a modifiable item. Thus, efforts are required to reduce sitting time and increase physical activity.
This study had limitations. As this was a cross-sectional study, only the correlation between problematic smartphone use and physical activity was confirmed, without elucidation of the causal relationship. Moreover, questions on physical activity were not taken from the Global Physical Activity Questionnaire, and only the number of days of exercise was presented, not the specific duration of each exercise. Regarding the question on high-intensity aerobic exercise and muscle strengthening exercise time, the response of 5–7 days a week was stated as ≥5 days a week, which accounts for the limitation in calculating the correct number of times that exercise was performed. Furthermore, there may be a lack of objectivity in the variables because the questions on the SES or academic performance of the study participants were answered subjectively by respondents without an objective standard.
Despite these limitations, it is meaningful to consider the relationship between smartphone use and physical activity using large-scale data representative of the youth in Korea.
In conclusion, by utilizing substantial data on Korean adolescents, this study confirmed a negative correlation between problematic smartphone use and physical activity. Furthermore, path analysis of the factors related to problematic smartphone use and engagement in physical activity revealed that several factors, including sex, SES, academic performance, and sitting time, directly and indirectly affected physical activity. Therefore, interventions aimed at improving these factors, implemented by individuals, schools, households, and local communities, could be advantageous in promoting a healthy lifestyle for adolescents who use smartphones. Further studies are needed to determine whether general treatment strategies for smartphone addiction can affect engagement in physical activity.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.