Barriers, Facilitators of Iron and Folic Acid Supplementation, and Deworming Program among School-Going Adolescents of Deoghar, Jharkhand, India: A Mixed-Methods Study
Article information

Abstract
Background
This study aimed to identify barriers and facilitators of iron and folic acid supplementation and deworming programs among school-going adolescents.
Methods
A mixed-method observational study was conducted among adolescents in the 8th to 10th standards and their teachers across four schools in Deoghar, Jharkhand, India, using simple random sampling. The study included a questionnaire on socio-demographics, knowledge (34 items) (α=0.894), attitudes (2 items) (α=0.711) toward iron deficiency anemia, awareness of the Weekly Iron and Folic Acid Supplementation (WIFS) program and deworming (20 items) (α=0.783), and practices related to iron folic acid supplementation (IFS) and deworming, along with qualitative components. Data were analyzed using jamovi.
Results
Compliance rates for IFS and deworming were 27.5% and 67.9%, respectively. The multivariable logistic regression analysis showed that sex, religion, caste, father’s educational status, per capita monthly family income (PCMI), diet type, adequate knowledge, and positive attitude toward anemia influenced IFS compliance. Religion, PCMI, and prior information on the importance of deworming facilitate compliance. Implementation barriers included irregular medication supply and a lack of student awareness.
Conclusion
Periodic evaluation, regular sensitization, and a consistent drug supply are necessary to effectively implement WIFS and deworming programs in the study area.
INTRODUCTION
Anemia is a widespread nutritional problem and significant public health concern among adolescents worldwide, particularly in developing countries. Iron deficiency anemia (IDA) was the second leading cause of years lost to death and disability among adolescents in 2019 [1]. Over the years, anemia among adolescents has increased, as indicated by the National Family Health Surveys (NFHS) conducted from 2005–2006 (NFHS-3) to 2019–2021 (NFHS-5). Anemia has increased from 55.8% to 59.1% among girls and 30.2% to 31.1% among boys, showing an alarming upward trend [2,3]. According to the recent NFHS report, the prevalence of anemia in the state of Jharkhand is significantly high, with rates of 65.8% among girls and 39.7% among boys, surpassing the national average [4].
To address the growing burden of adolescent anemia, the Ministry of Health and Family Welfare of India launched a Weekly Iron and Folic Acid Supplementation (WIFS) program in 2012 [5]. The program aimed to reduce the prevalence and severity of anemia among adolescents aged 10–19 years. Key interventions under the WIFS program include supervised weekly administration of 100 mg elemental iron and 500 μg folic acid (FA), utilizing a fixed day approach, screening and referral for anemia, biannual deworming with albendazole 400 mg, and provision of information and counseling services. The WIFS program is an evidence-based response designed to address anemia in teenage girls and boys [6-8].
However, achieving high coverage and sustained compliance with deworming programs presents challenges in regular drug administration, program coordination, and community participation [9-12]. Compliance with IFS and deworming is influenced by various personal, social, and environmental factors that influence compliance with FA supplementation and deworming. These factors encompass personal aspects such as knowledge about anemia, IFS, and parents’ education level; social elements, such as peer pressure and family support; and environmental components, such as timely tablet supply and social mobilization [13]. Despite the significance of compliance, studies conducted across the country have reported varying levels of adherence to the WIFS, ranging from 16.0% to 67.7%, with no specific literature available for the state of Jharkhand [14-18]. Considering this context, this study was undertaken to address this research gap.
Therefore, this study aimed to evaluate compliance levels, perceived barriers, and facilitators associated with the WIFS and deworming interventions among school-going adolescents and teachers in Deoghar, Jharkhand, India. By analyzing the current status and identifying specific challenges and enabling factors related to the implementation of these interventions in this context, this research aims to provide valuable insights for policymakers, program managers, and healthcare providers. These insights can be used to optimize the effectiveness of these interventions, ultimately leading to improved health and wellbeing of school-going adolescents in low-resource settings, such as Deoghar, Jharkhand, India.
METHODS
This mixed-method, cross-sectional, observational study was conducted among school-going adolescents and their teachers in Deoghar, a district nestled in the state of Jharkhand, India. The All-India Institute of Medical Sciences (AIIMS) in Deoghar is a prestigious medical institution in India, offering excellent healthcare, education, and research. With state-of-the-art facilities and expert staff, it serves the local community, meets healthcare needs, and provides accessible and cutting-edge medical care in Deoghar and its surrounding regions.
Based on a study conducted by Khapre et al. [14] in northern India, which reported a compliance rate of 16.0% for WIFS, the minimum sample size for our study was 841 participants. This calculation considered a 95% confidence level, relative precision of 20%, design effect of 1.5, and an anticipated response rate of 90%. The sample size was calculated using an online sample size calculator called Statulator [19]. The Deoghar District consists of 10 blocks in total of which, the Devipur and Deoghar blocks were selected for this study [20]. Devipur had nine school clusters with an average cluster size of 24 schools (range, 19–26 schools), whereas Deoghar had 17 school clusters with an average cluster size of 22 schools (range, 9–45 schools) [21,22]. Two school clusters were chosen from each study block. Within each selected school cluster (n=4), one coeducational school was selected. The selection process used simple random sampling with substitutes. Once permission was obtained from the relevant school authorities, the required sample size was determined for each selected school using a probability proportionate-to-size technique. Twelve random number lists (one for each school standard) ranging from one to 150 were generated using the OpenEpi random number generator [23]. Figure 1 depicts the geographical location of the study area.
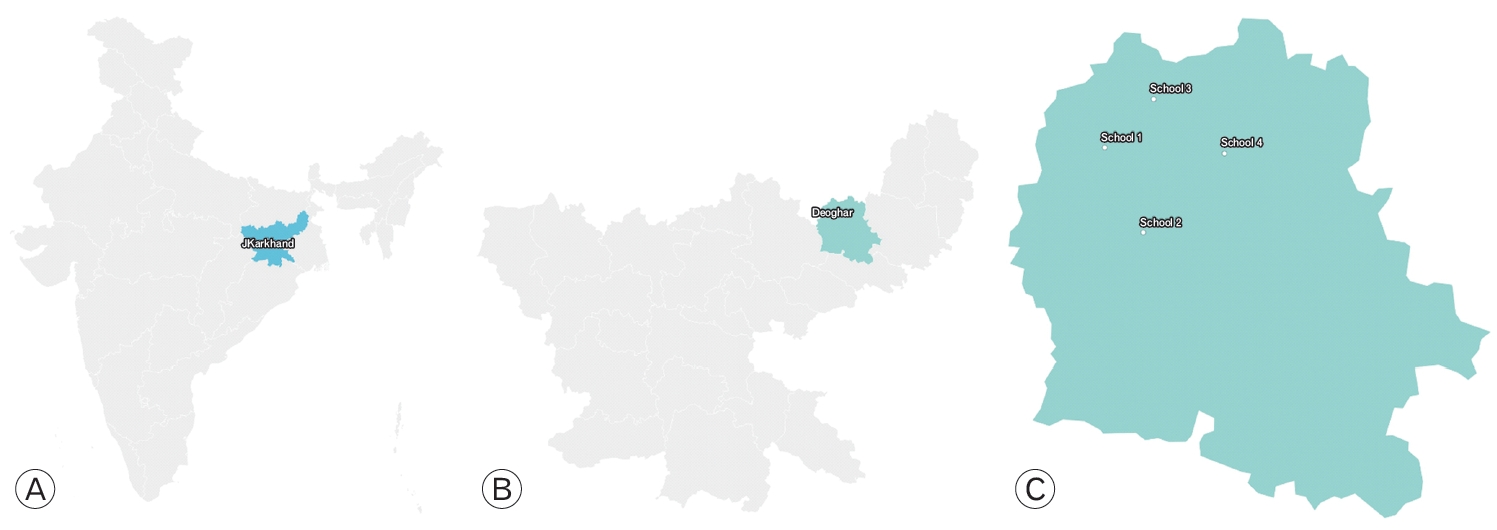
Map showing location of the study area. (A) Map of India showing the location of Jharkhand State. (B) Map of Jharkhand State showing the location of Deoghar District. (C) Map of Deoghar District showing the positions of the study schools.
On the day of data collection, the students were approached based on a specific random number list, which corresponded to their roll numbers. Additionally, group discussions were conducted with students and teachers gathering their perceptions of barriers and facilitators related to the implementation of the program at school level. Prior to the discussions, informed consent was obtained from all participants, and audio recordings were made to ensure accurate documentation of the conversations. These group discussions provided valuable insights into the experiences and viewpoints of both students and teachers, shedding light on specific factors influencing the implementation of the program in school settings.
The quantitative portion of the survey comprised a multi-section questionnaire. First, sociodemographic information was collected to understand participants’ background characteristics. Second, the knowledge section comprised 34 items that assessed participants’ understanding of the IDA. The reliability analysis (Cronbach’s α) for this section yielded a value of α=0.894, indicating good internal consistency. Third, the questionnaire included two items to gauge the participants’ attitudes toward the IDA. The reliability analysis for the attitude section yielded an alpha value of α=0.711, indicating acceptable internal consistency. The final questionnaire contained 20 items focused on assessing the participants’ awareness of WIFS and deworming, as well as their practices related to WIFS. The reliability analysis for this section yielded a value of α=0.783, indicating satisfactory internal consistency. Figure 2 represents the conceptual model of IFS compliance based on a previous study conducted by Gosdin et al. [24].
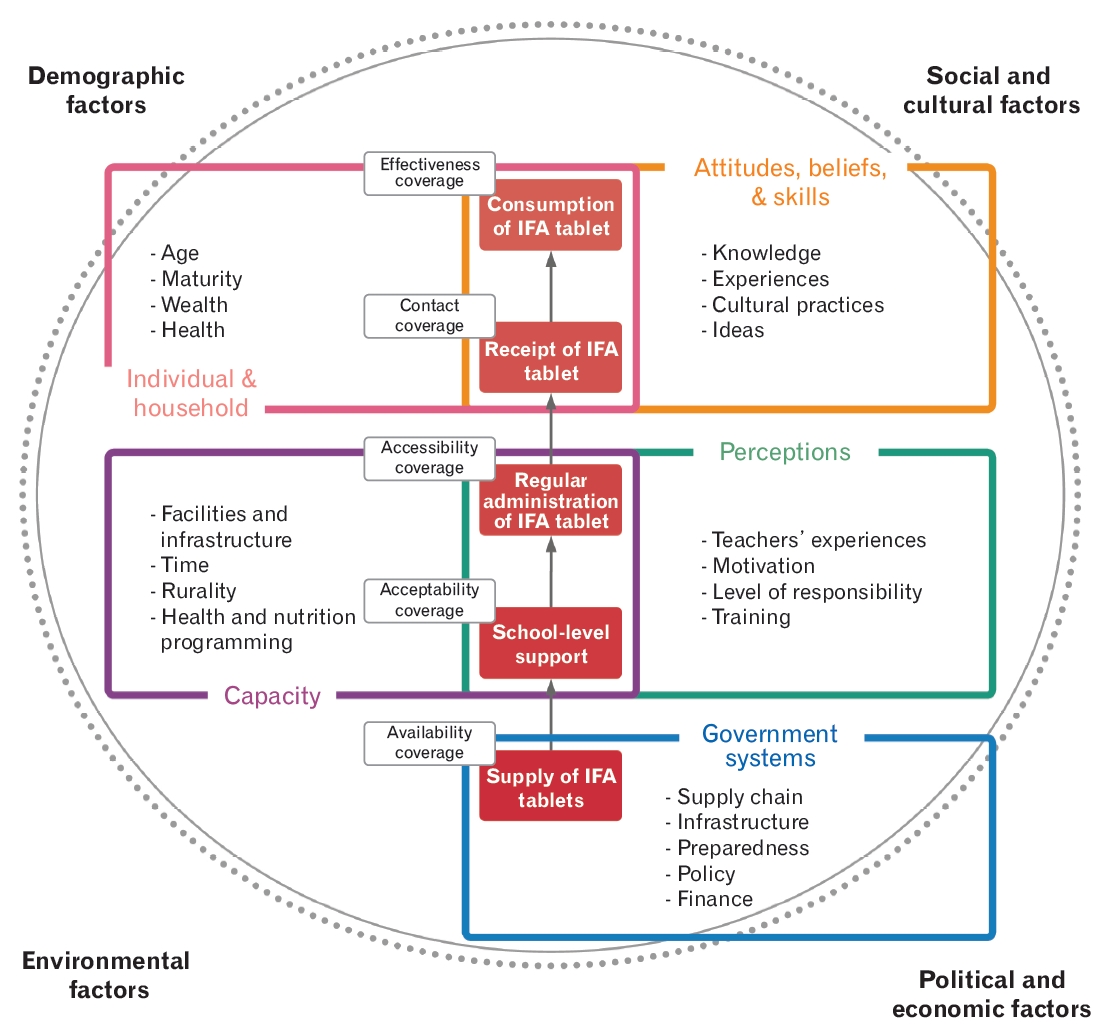
Conceptual framework of the barriers to and facilitators of school-based iron and folic acid (IFA) supplementation. This framework incorporates elements from Tanahashi’s levels of health service coverage (1978) and the Innocenti Framework (UNICEF, 2018)[24].
This study employs specific definitions of various aspects. Participants who had consumed at least two tablets of iron and folic acid (IFA) and albendazole within the previous year were categorized as compliant with IFS and deworming, respectively. We investigated biannual (6-monthly) instead of weekly adherence to IFS because the study schools did not have a weekly supply of IFA. Instead, IFA was provided irregularly in conjunction with deworming tablets in most schools. To determine the overall knowledge scores regarding IDA-related information, the WIFS, and deworming, the individual scores for all relevant items (34 for IDA and 20 for the WIFS and deworming) were summed up, with one point awarded for each correct response. When assessing attitudes toward anemia, two items were evaluated: vulnerability to anemia (not likely, 0; not sure, 1; likely, 2) and perceived severity of anemia (not serious, 0; not sure, 1; serious, 2). Participants who had achieved scores of 14 or higher were considered to possess satisfactory knowledge of IDA (median, 14; maximum score, 33; minimum score, 0), whereas scores of 9 or higher indicated satisfactory knowledge of WIFS and deworming (median, 9; maximum score, 20; minimum score, 3). Additionally, individuals who scored 3 or higher were regarded as having a favorable attitude toward anemia (median, 3; maximum score, 4; minimum score, 0).
The study protocol (Ref: 2023-83-IND-02, dated January 30, 2023) were approved by the Institutional Ethical Committee of the AIIMS, Deoghar, Jharkhand, India. Written informed consent was obtained from each participant before enrollment in the study. Throughout the process of data collection, entry, analysis, and reporting, the confidentiality and anonymity of participants were ensured.
Categorical variables are represented as proportions and percentages, whereas continuous variables are reported as either mean with standard deviation (SD) or median with interquartile range (IQR) depending on their distribution. The significance of the attributes related to compliance with the IFS and deworming was assessed using the chi-square test of association. Variables that showed significant associations with IFS and deworming compliance in the bivariate analysis were included in the multivariate logistic regression analysis. Two separate multivariate logistic regression models were developed using the forced entry method to examine the multiple factors influencing compliance with IFS and deworming. The strength of the association was quantified using odds ratios (OR). A confidence level of 95% was used for all the statistical analyses. Data analyses were conducted using jamovi ver. 2.3.26 (https://www.jamovi.org/) [25]. Qualitative data analysis initially involved transcribing group discussions in Hindi, which were then translated into English. Transcripts were systematically analyzed by the study investigators to identify common themes and patterns related to the reported barriers and facilitators. Participants’ verbatim quotes and statements were organized thematically to provide a comprehensive representation of their perspectives and experiences.
RESULTS
1. Findings of the Quantitative Survey among School-Going Adolescents
The study involved individuals with an average age of 14.6 years (SD=1 year), ranging from 12 to 18 years. The median education level was 8 years (IQR, 0–10 years) for fathers and 5 years (IQR, 0–8 years) for mothers. The participants’ families had a median per capita monthly family income (PCMI) of 15.3 US dollars (USD) (IQR, 10.2–21.4 USD). Among the surveyed students, 88.4% received IFS, of whom 63.6% received it biannually, and 24.8% received it annually. Overall, 67.9% of the participants reported consuming school-provided IFA. The most common time for IFS consumption was at any time (55.4%), followed by after (37.5%) and before meals (7.1%). Among those who reported consuming IFA (n=586), 39.6% (27.5% overall) took two tablets, 23.7% took one tablet, and 36.7% had not taken any tablets within the past year. Most students (93.4%) consumed IFS tablets in front of their teachers. Regarding compliance with biannual deworming, 86.0% of participants reported consuming albendazole at some point. In the previous year, 67.9% had taken two tablets, 16.3% took only one tablet, and 15.9% had not taken any.
Compliance with IFS was influenced by various factors including age, sex, reading proficiency, caste, religion, parents’ education level, PCMI, dietary habits, knowledge about IDA, WIFS, and deworming, as well as information on the importance of IFA intake and its side effects. Similarly, compliance with deworming was affected by age, sex, religion, parents’ education level, PCMI, dietary habits, knowledge about IDA, and information about the importance of deworming. Among the study participants, teachers (74.0%) were the primary source of knowledge on IDA, WIFS, and deworming, followed by other family members (43.4%), parents (38.1%), books (28.4%), television (21.9%), newspapers (19.9%), and friends (17.7%) (Table 1).

Distribution of the school-going adolescents as per their background characteristics, iron folic acid supplementation, and deworming compliance (n=843)
Table 2 presents the univariate and multivariate attributes associated with compliance with IFS and deworming. The independent variables in the IFS compliance model accounted for 26.5% of the variability in outcomes, with a predictive accuracy rate (PAR) of 79.0%. Similarly, the independent variables in the deworming compliance model explained 28.7% of the variability in outcomes, achieving a PAR of 75.4%. The reasons for not consuming IFS were primarily a lack of information (36.0%) and non-availability (32.9%), followed by concerns over side effects (22.3%). Other factors included a lack of perceived need (17.1%), feeling full (10.8%), poor packaging (9.7%), metallic taste (9.2%), darkening of the stool (7.9%), parental restrictions (6.2%), constipation (1.3%), abdominal pain (1.3%), and nausea (1.3%). However, noncompliance with biannual deworming was attributed to a lack of perceived need (46.1%), fear of side effects (39.5%), and a lack of information (38.4%).

Univariate and multivariable logistic regression analysis showing attributes affecting iron folic acid supplementation and deworming compliance among school-going adolescents (n=843)
2. Key Findings of Group Discussions with Students and Teachers
The perceived barriers and facilitators identified by students and teachers are summarized in Table 3.
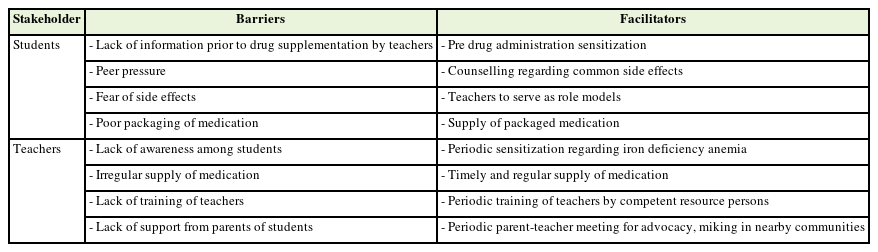
Summary of the perceived barriers and facilitators of iron & folic acid supplementation and deworming program as per students and teachers
1) Lack of Information prior to drug supplementation
One male student from School 1 said, “We were not told what these medications are given for. Teachers just give it to us and ask us to consume.” This issue was raised by several other students in the schools. One female student from School 3 said, “If I am told what these medications are given for, I will definitely consume them.” The other students who were present during the conversation agreed with her. One male student from School 1 said, “If our teachers consume the drugs in front of us then we will feel more confident about taking them.” Students at other schools shared similar opinions.
2) Peer pressure
A male student from School 4 said, “My friend told me if you take medicine for worms (albendazole), they will come out from your mouth, block breadth, and you may die.” One female student from School 2 said that “one of my friends told me if you take iron tablet frequently then your skin will be blackened and no one will marry you, so I decided not to take it.” Similar results have been reported previously.
3) Fear of side effects
One male student at School 2 said, “when last time I took the drugs (IFA), I had black hard stools the next day, I was so scared and decided not to take them anymore.” Students from other schools also reported similar events. One female student at School 2 said, “Sometimes teachers scold us if we ask questions about side effects of the given drugs, so I just take the drugs and throw them away when they are not observing.”
4) Poor packaging of medication
A female student from School 1 stated that “Some medications given to us are not packaged (albendazole), so I am doubtful about its safety. I cannot check for its expiry date, so I commonly throw them.” She also said, “If the Government is so concerned about our health, they should at least pack them properly before giving it to us.” Students from other schools have also raised this concern.
5) Lack of awareness among students
One teacher from School 4 said, “There is a lack of awareness regarding khoon-ki-kami (anemia) among students, we try to teach them but sometimes they forget it.” For this he has suggested “I feel there should be periodic sensitization of students regarding anemia and benefits of iron and deworming tablets.” Most other teachers from the same and other schools had similar perceptions.
6) Irregular supply of medication
A teacher from School 3 said, “Before coronavirus disease 2019 (COVID-19) we regularly used to get iron and albendazole tablet, but that was biannual not weekly. Weekly IFA was once provided for girl students a few years ago for few months. After COVID-19, although we get biannual albendazole regularly, the iron supply is quite irregular, sometimes they give, sometimes not.” All teachers from the other schools reported similar results. A teacher from School 1 said, “We have no problem in giving iron and albendazole tablets as the government supplied it regularly to our school until now. A teacher must go to the community health center to collect it. For that, others face difficulty as we have very little manpower with plenty of work to do. We do not have time for all this.”
7) Lack of training
A teacher from School 2 said, “We are trained regarding this program by teachers like us only. who I feel is not competent enough to train us.” He suggested that “periodic training (at least once a year) of all the teachers on rotation should be done by competent persons (i.e., doctors, nurses, etc.).” Teachers from different schools agreed.
8) Lack of support from parents of students
One teacher from School 3 said, “Everyone (specially parents of the students) have a common belief that whatever is supplied by the government is of inferior quality, so they ask their wards not to consume the iron and deworming tablets provided at school.” In this context, he has also suggested that “There should be periodic parent–teacher meetings to sensitize them about benefits of the provided tablets.” Another teacher said, “If regular parent–teaching meeting is not possible, benefits of consumption of iron and deworming tablets should be done in the nearby communities.”
DISCUSSION
The primary focus of this study was to investigate the adherence to and factors affecting the consumption of iron and deworming tablets among school-going adolescents. Additionally, the research aimed to gain insight into the perceived barriers and facilitators experienced by both students and teachers in the study schools.
In this study, the overall compliance rate with IFS among students was 27.5%. This percentage is significantly lower than previous Indian studies by Khapre et al. [14] (45%), Priya et al. [18] (47.2%), Ansari et al. [16] (62.0%), Wangaskar et al. [15] (67.7%), and Sau et al. [17] (67.7%). In addition, it was lower than the compliance rate reported by Gosdin et al. [24] (56.0%) in a study conducted in Nigeria by Gosdin et al. [24] (56.0%). However, this was higher than that reported in a study conducted in Ghana by Dubik et al. [26] (26.2%). Importantly, the findings of our study are not directly comparable to those of previous studies. Except for Khapre et al. [14] (who reported both weekly and 3-monthly compliance) and Gosdin et al. [24] (who reported compliance at 15 weeks), the other studies primarily focused on WIFS compliance. In contrast, our study specifically explored the biannual (monthly) compliance with IFS since the study schools did not have a weekly supply of IFS. In certain instances, the supply of IFS was irregular or non-existent, as reported by certain schools. Such a situation is unacceptable, particularly considering alarming statistics that reveal that approximately two-thirds (65.8%) of teenage girls and two-fifths (39.7%) of teenage boys in Jharkhand are anemic. In terms of compliance with biannual albendazole, a significant proportion of the students (67.9%) were adherent, which is consistent with the findings of Dhupdale et al. [27] (61.3%).
Regarding various factors influencing IFS compliance, this study identified that parents’ education level, knowledge about IDA, and awareness of the importance of deworming were key attributes. These findings are consistent with the observations from a systematic review conducted by Silitonga et al. [13] and studies conducted by Dubik et al. [26] and Gosdin et al. [28]. In our study, older age and male were associated with greater IFS compliance, which aligns with the findings of Wangaskar et al. [15] We observed that among various castes excluding scheduled castes (SC)/scheduled tribes (ST), a higher adherence presented to both IFS and deworming. This could be attributed to a potential lack of awareness among individuals with SC/ST regarding the benefits of IFS and deworming. Nonvegetarians exhibited greater compliance with both the IFS and deworming. Hindus demonstrated a higher level of adherence to deworming, whereas Muslims showed a greater commitment to IFS. It is important to note that the proportion of vegetarians and Muslims represented only one-tenth of the study population, which is notably lower than India’s national average [29,30]. Therefore, further research with a more representative sample is necessary to draw conclusions regarding these associations. Fear of side effects emerged as a significant barrier to the implementation of the IFS program, similar to the studies by Sau et al. [17] and Ansari et al. [16] The irregular supply of medication was identified as a key factor affecting the implementation of the IFS program by Khapre et al. [14], which aligns with our own observations. Among the factors influencing IFS and deworming compliance and implementation, a lack of information regarding IDA, WIFS, deworming, lack of community support, and irregular drug supply were the major modifiable attributes that implementers and policymakers should address. Sociodemographic attributes were mostly non-modifiable, except for socioeconomic status.
Efforts should focus on improving compliance by educating students, teachers, and parents about the critical importance of regular consumption of IFS and deworming. It is essential for school teachers to receive periodic training on WIFS and deworming, accompanied by regular assessments of their training needs. To monitor progress and overcome barriers to compliance, it is crucial for independent assessors to conduct regular evaluations and assessments using predefined checklists. Sensitization campaigns should be organized both within schools and in the community to increase awareness and address misconceptions. These campaigns should actively involve students and their parents in fostering a sense of ownership over the program. Finally, ensuring a consistent supply of medications and improving coordination among stakeholders were fundamental to the success of the program.
This study has several limitations. First, self-report measures were used, which may introduce recall or social desirability bias, potentially affecting data accuracy. Second, the study focused on a specific age group and geographical area, limiting the generalizability of the findings to other populations or settings. Third, it primarily relied on quantitative surveys and group discussions, neglecting the perspectives of other stakeholders such as parents or healthcare providers. Fourth, this study did not consider the long-term effects of compliance, and future research should explore their impact on health outcomes. Additionally, potential interactions between factors influencing compliance were not investigated, which could provide a more comprehensive understanding. Despite these limitations, this study offers valuable insights into compliance and factors influencing the consumption of iron and deworming tablets among school-going adolescents, exploring the perceived barriers and enablers of the program from the perspectives of both beneficiaries and school-level providers.
In conclusion, the findings revealed a notable disparity in compliance rates for IFS among study participants, demonstrating a significant deviation from the findings in the existing literature. However, deworming compliance was comparatively satisfactory. To improve compliance, the education of students, teachers, and parents should be prioritized regarding the importance of consistent IFS consumption and deworming. Organizing sensitization campaigns that actively involve students, parents, and communities can effectively increase awareness, address misconceptions, and foster a sense of program ownership. It is vital to ensure a consistent supply of medication and enhance coordination among stakeholders to ensure the successful implementation of the program.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We extend our sincere gratitude to the students and teachers who participated in this study. Their voluntary participation and cooperation were essential for the success of this project.