INTRODUCTION
Generalized anxiety disorder (GAD) is characterized by chronic anxiety and excessive worry in a variety of situations. According to the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition, GAD involves excessive concerns about everyday situations, heightened tension, and physical symptoms. These symptoms can diminish the quality of life and must persist for at least 6 months before diagnosis [1].
Individually, GAD can reduce a person’s quality of life and affect their physical health and relationships [2]. Socially, it can reduce job performance and social participation, and nationally, it can have effects such as increased healthcare costs and decreased productivity [3]. According to a recent report from the Korean Ministry of Health and Welfare, the lifetime prevalence of GAD in Korea was 1.7%, with a 1-year prevalence of 0.4% [4].
Recent data released by the Korea Health Insurance Review and Assessment Service indicate a notable increase in the number of patients with anxiety. Between 2017 and 2021, there was a 32% increase in anxiety cases, totaling 875,108 individuals. Studies have investigated the association between tobacco use and GAD. However, in Korea, only a few studies with small numbers of participants have reported an association between tobacco use and the severity of anxiety symptoms [5].
Recently, the global use of noncombustible nicotine or tobacco products (NNTPs) has increased. According to Organization for Economic Cooperation and Development health data from 2021, Korea’s NNTP usage rate is 5.9%, ranking it as the third-highest country in the world [6]. Nevertheless, no studies have been conducted on the association between NNTP use and GAD in Korean adults. Therefore, we investigated the association between tobacco status and GAD using extensive population data from the Korea National Health and Nutrition Examination Survey (KNHANES).
METHODS
1. Data Source
This study was based on data from the KNHANES VIII (2021). The KNHANES has been conducted in South Korea since 1998 by the Division of Chronic Disease Surveillance of the Korea Disease Control and Prevention Agency (formerly, Korea Centers for Disease Control and Prevention) and the Korean Ministry of Health and Welfare. This population-based cross-sectional survey employs stratified multistage probability sampling units based on geographical area, sex, and age, which are determined from the household registries of the National Census Registry, and assesses the health and nutritional status of the nationwide Korean population. The survey consists of questionnaires regarding the participants’ health interviews, health examinations, and nutrition. The Institutional Review Board Committee of Korea University Hospital exempted this study from informed consent because it utilized publicly available data provided by KNHANES 2021. As this study employed a retrospective design using publicly accessible data, the requirement for informed consent from individual patients was omitted.
2. Study Population
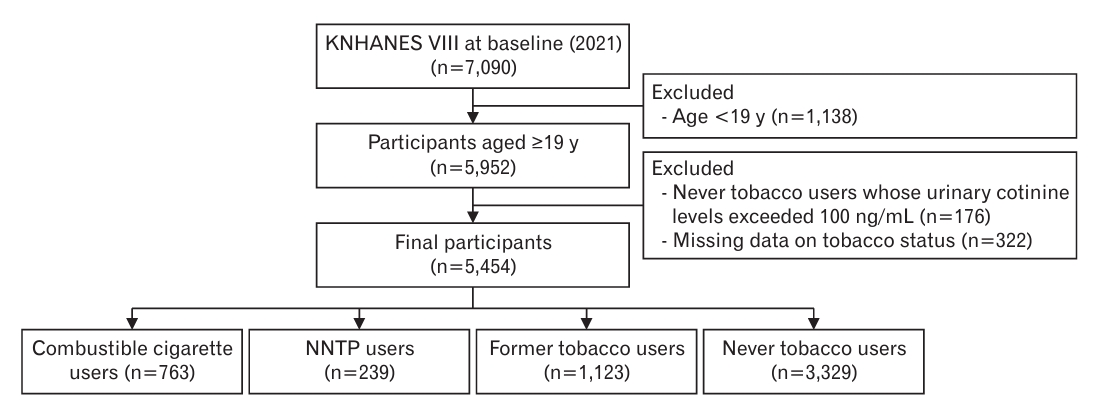
This study examined data obtained from a representative sample from the KNHANES VIII (2021). The data were limited to 2021, because the Generalized Anxiety Disorder-7 (GAD-7) surveys were conducted only during that year. As shown in Figure 1, the study population included Koreans (n=7,090) who completed a health checkup survey. Individuals under 19 years of age (n=1,138), for whom tobacco use is legally prohibited, were excluded. Among the participants aged 19 years and older (n=5,952), those who reported being never tobacco users (n=3,329) but had a urine cotinine level of 100 ng/mL were excluded (n=176). In addition, participants with missing GAD-7 (n=322) or tobacco status data were excluded. Finally, 5,454 adults were included in the analysis.
3. Definitions of Tobacco Status
The “combustible cigarette smoker” was defined as an individual who has smoked more than 100 combustible cigarettes in their lifetime, currently smoke combustible cigarettes, and do not currently use NNTPs, including heated tobacco products or electronic (e)-cigarettes [7]. The “NNTP only users” was defined as an individual who currently uses only NNTPs, including heated tobacco products or e-cigarettes, and do not currently use combustible cigarettes. The “combustible cigarette and NNTP user” was defined as an individual who has smoked more than 100 combustible cigarettes in their lifetime, currently smokes combustible cigarettes, and currently uses NNTPs. The “NNTP user” includes both NNTP only users and combustible cigarette and NNTP users. The “former tobacco user” was defined as an individual who has smoked more than 100 combustible cigarettes in their lifetime and has used NNTPs, including heated tobacco products or e-cigarettes, but does not currently use either. The “never tobacco user” was defined as an individual who has smoked fewer than 100 combustible cigarettes in their lifetime or has never smoked at all and has never used NNTPs, including heated tobacco products or e-cigarettes.
4. Definition of Generalized Anxiety Disorder
The GAD-7 questionnaire, which consists of seven questions, is a widely used screening tool for GAD [8,9]. Participants subjectively evaluate anxiety-related symptoms for each question and are assigned scores ranging from 0 to 3 based on personal experiences. GAD-7 total scores are categorized as follows: 0–4 points indicate minimal anxiety, 5–9 points suggest mild anxiety, 10–14 points imply moderate anxiety, and 15 or higher points signify severe anxiety. A score of 10 or higher indicates a high risk of GAD, with a reported sensitivity of 89% and specificity of 82% for diagnosing GAD. We used a cutoff value of 10 to determine the prevalence of GAD within our sample [10-12].
5. Covariates
Participants in the KNHANES were asked about their demographic and social lifestyle factors and medical conditions. These factors included sex, age, education, household income, urban residence, marital status, occupation, alcohol or cigarette use, and a confirmed diagnosis of any comorbidities. Participants were asked about their highest level of educational attainment. Those with a high school diploma or higher were identified as the highly educated group. Monthly household income was divided into quartiles, and those in the lowest quartile were identified as the lower-income group. Additionally, the participants were categorized into two groups based on their residential location, marital status, and occupational status at the time of the survey. Body mass index was determined by dividing weight (kg) by the square of height (m) and classified according to Asian standards into different categories: normal (18.5–22.9 kg/m2), pre-obese (23–24.9 kg/m2), and obese class I–III (≥25 kg/m2). The history of certain comorbidities was determined by answering “yes” to questions regarding the diagnosis of specific diseases. These diseases include hypertension, type 2 diabetes, dyslipidemia, cardiovascular diseases, stroke, and rheumatism. Psychosocial factors were analyzed, including variables such as perceived high stress, depressive mood lasting for more than 2 weeks, and experiencing suicidal thoughts within the past year. Urine cotinine levels were measured using gas chromatography-mass spectrometry with a Perkin Elmer Clarus 600 T detector (Perkin Elmer, Turku, Finland).
6. Statistical Analysis
Data from the KNHANES were extracted using a complex sampling design, specifically, a two-stage stratified probability sampling method. This design incorporates elements such as strata, clusters, and weights. To ensure the representativeness of the sample and accurate variance estimation, the analysis considered missing data and the incorporation of weights, strata, and cluster elements. For statistical analysis, the Rao-Scott chi-square test was used for categorical data, whereas t-tests were used for continuous data. When the outcome variable was nominal, a generalized logistic model, specifically the generalized logit model, was used for the analysis. Multivariate-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using multiple logistic regression to evaluate the association between tobacco use and GAD. Model 1 was analyzed after adjusting for sex and age. Model 2 was analyzed after adjusting for general characteristics, including educational level, household income, residential location, marital status, and occupational status. KNHANES data were analyzed using the SAS ver. 9.3 (SAS Institute Inc., Cary, NC, USA) to reflect the complex sampling design and sampling weights of the KNHANES and represent Korean population estimates. Two-tailed P-values of <0.05 were considered statistically significant.
RESULTS
1. Baseline Characteristics Based on Tobacco Status
Table 1 presents an overview of the characteristics based on tobacco status: combustible cigarette smokers (n=763, 14.0%), NNTP users (n=239, 4.4%), former tobacco users (n=1,123, 20.6%), and never tobacco users (n=3,329, 61.0%). The mean age was 46.6 years for combustible cigarette smokers, which was higher than the mean age (37.1 years) of NNTP users (P<0.0001). The group aged 50 years or older had the highest proportions of NNTP users and never tobacco users (P<0.0001). The highest proportion of NNTP users was found among those aged 19–29 years (P<0.0001). Higher proportions of individuals with a high education level, high household income, urban residency, and employment were found among NNTP users than among combustible cigarette smokers and never tobacco users (all P<0.001). Former tobacco users comprised the highest proportion of married individuals (P<0.001). Both combustible cigarette smokers and NNTP users exhibited significantly higher rates of experiencing high stress and depressive mood for over 2 weeks than never tobacco users (P<0.0001). Never tobacco users exhibited a lower prevalence of obesity and a smaller proportion of heavy drinkers than combustible cigarette smokers and NNTP users (P<0.0001).
2. Prevalence of Generalized Anxiety Disorder according to Tobacco Status
As shown in Table 2, the prevalence of GAD was 5.8% among combustible cigarette smokers and 4.8% among NNTP users. The prevalence of GAD was 3.1% in former tobacco users and 4.1% in never tobacco users. However, there was no statistically significant difference in GAD prevalence among the four groups (P=0.0521).
3. Association between Tobacco Status and Generalized Anxiety Disorder
Table 3 shows the results of the multivariable logistic regression analyses performed to examine the relationship between tobacco status and GAD. In model 1, the adjusted OR for GAD in the combustible cigarette smokers, compared to the never tobacco users, was 2.79 (95% CI, 1.72–4.55), and the adjusted OR for GAD in the NNTP users was 2.09 (95% CI, 1.16–3.75). However, there was no significant association with GAD in former tobacco users (OR, 1.63; 95% CI, 0.98–2.72). In model 2, the adjusted OR for GAD in combustible cigarette smokers compared to never tobacco users was 2.74 (95% CI, 1.66–4.50) and the adjusted OR for GAD in NNTP users was 2.11 (95% CI, 1.16–3.83). However, in the former tobacco users, there was no significant association in OR for GAD when compared to never tobacco users (OR, 1.63; 95% CI, 0.98–2.72). In addition, we examined the association between combustible cigarettes and NNTP, NNTP only, and GAD (Supplement 1). The use of NNTP only was associated with an increased risk of GAD (OR, 2.67; 95% CI, 1.39–5.12). Supplement 2 shows the association between tobacco use and GAD according to sex. Women who smoked combustible cigarettes had a significantly higher risk of developing GAD (P<0.05).
4. Subgroup Analysis
We performed stratified analyses according to sex, age, education level, household income, residential location, marital status, occupational status, obesity, alcohol consumption, mental health (perceived stress, depressive mood, and suicidal thoughts), comorbidities, hypertension, diabetes mellitus, dyslipidemia, cardiovascular disease, stroke, and rheumatism) (Table 4). The association between combustible cigarette smokers and GAD did not differ across most subgroups, including sex, age, education level, household income, residential location, marital status, obesity, alcohol consumption, depressive mood, suicidal thoughts, hypertension, diabetes mellitus, and dyslipidemia (P for interaction=0.240, 0.809, 0.681, 0.261, 0.283, 0.793, 0.315, 0.599, 0.325, 0.374, 0.236, and 0.978, respectively) but did differ for some subgroups including occupational status, perceived stress, cardiovascular disease, stroke, rheumatism (P for interaction=0.018, <0.001, <0.001, <0.001, and <0.001, respectively).
DISCUSSION
Our results revealed that within the adult population in South Korea, in both combustible cigarette smokers and NNTP users, tobacco use was significantly associated with GAD compared to never tobacco users. However, among former tobacco users, there was no significant association with GAD when compared to never tobacco users.
Reviewing previous studies on the correlation between tobacco use and anxiety, Morissette et al. [13] indicated that combustible cigarette smoking increases the risk of developing anxiety disorders later, whereas Taylor et al. [14] reported that quitting smoking is associated with a reduction in anxiety compared with continuing to smoke. Zvolensky et al. [15] provided evidence of a positive association between anxiety and e-cigarette use.
A review article by Moylan et al. [16] mentioned that the association between tobacco use and anxiety may be linked to various pathways, including neurotransmitters, neurobiology, respiratory health, and autonomic regulation. However, research on the association between combustible cigarette smoking and GAD has been conducted only in specific generations or with small populations within Korea [17-19]. However, our study is the first nationwide investigation to explore the association between tobacco use and GAD among Korean adults, rather than specific generations.
Recently, Kim et al. [20] examined the motives for e-cigarette use using data from the 6th KNHANES. According to their findings, 41.5% of participants believed that e-cigarette use could assist in quitting smoking, and 18.5% perceived e-cigarettes as less harmful than combustible cigarettes [20].
According to research conducted in the United States, e-cigarette users were found to have a 39% higher risk of developing chronic respiratory conditions (such as chronic bronchitis, chronic obstructive pulmonary disease, pulmonary fibrosis, and asthma) than never tobacco users [21]. In another study, e-cigarette users were found to have a 1.8 times higher risk of myocardial infarction than never tobacco users, which was slightly lower than the 2.7 times higher risk observed in daily combustible cigarette smokers [22,23]. Despite various research findings indicating the health risks of e-cigarettes, there is a tendency for people to overlook such hazards. Our results indicate that both NNTP users and combustible cigarette smokers have significantly higher odds of developing GAD than never tobacco users, although no significant association was observed between former tobacco use and GAD. Therefore, quitting not only combustible cigarette smoking but also NNTP use is important.
Our study has some limitations. First, the data were limited to 2021 because the GAD-7 surveys were conducted in 2021. Second, the GAD-7 questionnaire was used to assess GAD instead of a structured psychiatric interview, potentially leading to an underestimation of GAD prevalence owing to its self-reporting nature. Third, this study used a cross-sectional design to analyze a sample of the general population. Therefore, causal relationships could not be explored. Nonetheless, a strength of this study is the analysis of data from a large-scale national survey, the KNHANES, which are representative of the Korean population.
In conclusion, regardless of the type of tobacco (NNTPs or combustible cigarettes), tobacco use was positively associated with GAD. However, there was no significant association between the former use of tobacco and GAD. Based on these findings, tobacco use can serve as a triggering or exacerbating factor for individuals who frequently experience anxiety and could effectively motivate them to contemplate quitting not only combustible cigarette smoking but also NNTP use. Additionally, it is crucial to pay attention to screening for GAD and implement appropriate early interventions.