INTRODUCTION
New knowledge is continuously created in medicine. Therefore, continuing medical education is critical, and conferences are one of the most useful methods of providing this education.1,2) Doctors and residents in family medicine require continuous education and clinical experience in a variety of specialties. Conferences are mandatory in residency programs. Nevertheless, family medicine departments of many hospitals find it difficult to hold regular, independent conferences.3) Frequency of conferences decreases when a family medicine department has a smaller body of residents and staff.4) Seoul National University Bundang Hospital Department of Family Medicine (SNUBHFM) was established in 2009 with three staff members and no residents, and was unable to hold regular conferences for a year. Kangwon National University Hospital Department of Family Medicine (KNUHFM) has six residents and two staff members, and experienced similar difficulties as SNUBHFM. In contrast, Seoul National University Department of Family Medicine (SNUHFM) holds regular conferences, which are facilitated by many physicians of SNUHFM (6 staff members, 14 fellows, 57 residents).
CASE REPORT
1. Participants and Period of Joint Videoconferences
Joint videoconferences were conducted from April 1 to October 29, 2010. During that period, 6 professors, 14 fellows and 57 residents from SNUHFM, 3 professors and 1 fellow from SNUBHFM, and 2 professors and 6 residents from KNUHFM participated in joint videoconferences.
2. Joint Videoconferences
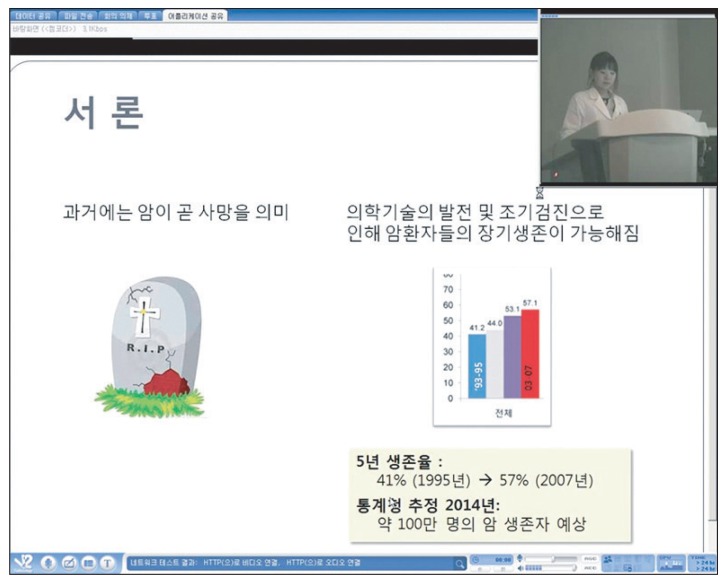
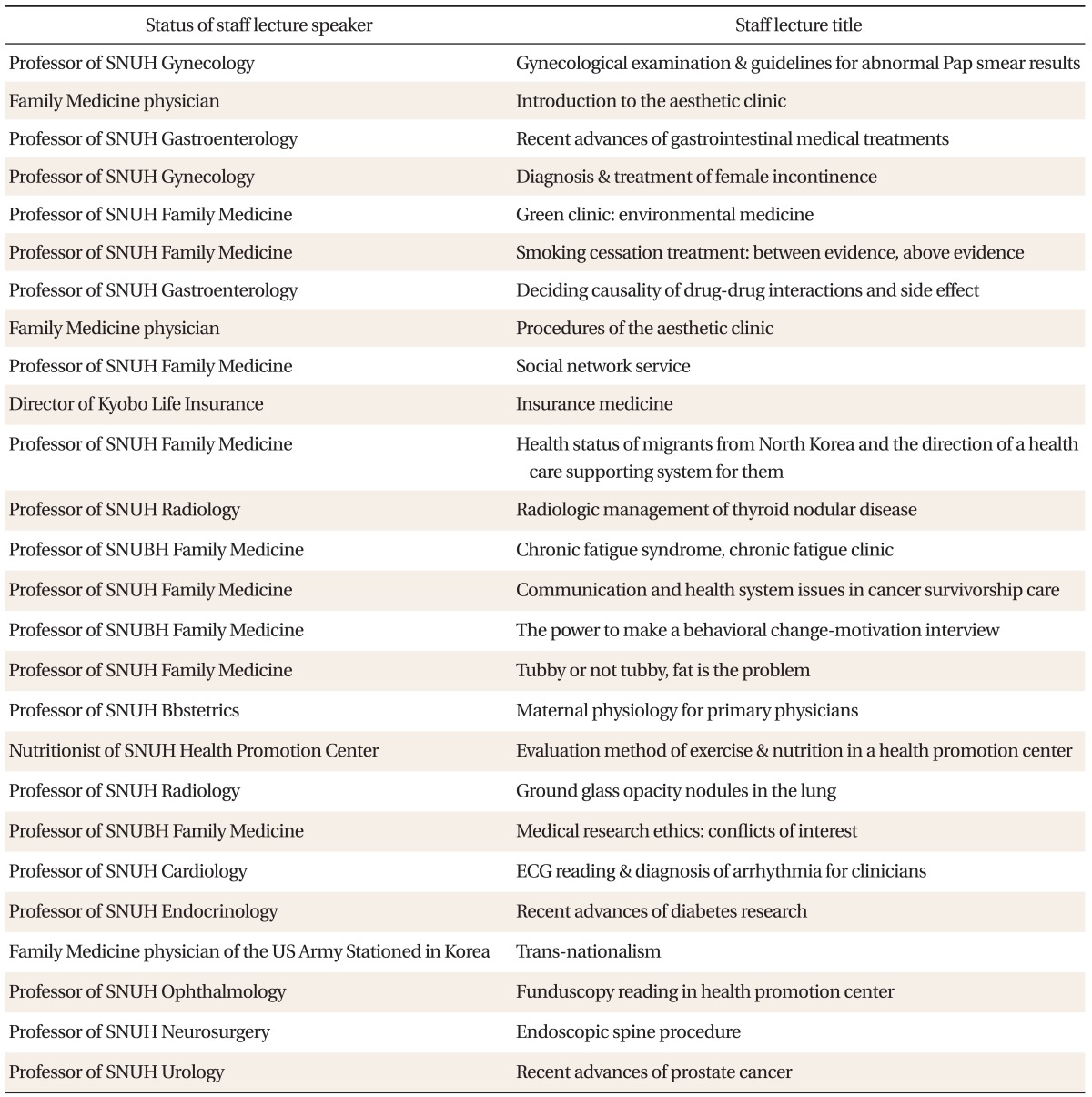
Departments of family medicine of the three hospitals shared conferences in the mornings using a videoconferencing system. Each hospital took turns to make a PowerPoint presentation at each conference, and the other hospitals watched the presentation via internet in real time. After the presentation, all three hospitals participated in feedback and discussion through the videoconferencing system. Eighty-one joint videoconferences were held during the period. These conferences included 39 clinical review presentations, 16 journal reviews and 26 staff lectures (Table 1). Seventy-nine morning conference presentations were given by SNUHFM, while SNUBHFM held three staff lectures. PowerPoint slideshows were transferred to the other two locations in the same resolution as presenter's monitor, and the images and voices of the speaker were transmitted in real time in acceptable quality (Figures 1-5).
3. Software and Hardware
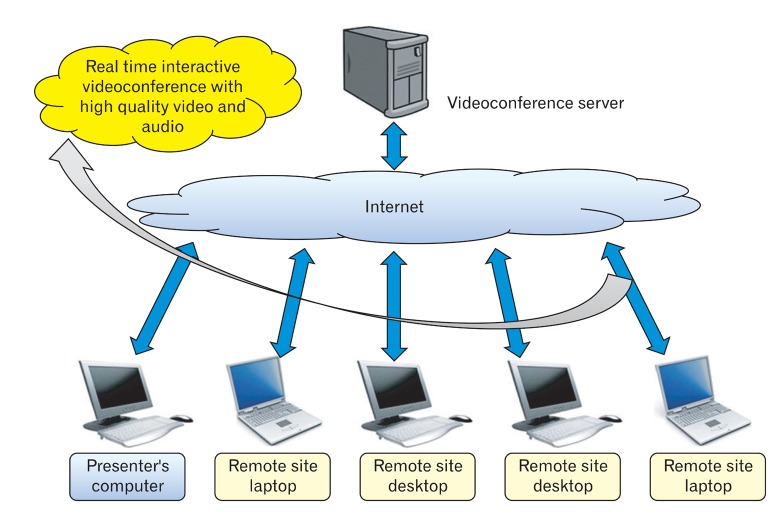
We used videoconferencing software (V2 conference; V2 Technology, Beijing, China) installed in the Seoul National University College of Medicine. V2 Conference is a web-based client-server system that allows up to 300 parties to participate in a video-conference simultaneously (Figure 6).
We used highly sensitive microphones (ETM-003; Edutige, Seoul, Korea) and an echocanceler (XING; IPEVO, Taipei, Taiwan) for audio communication and video cameras (VC-03; Canon, Tokyo, Japan) for video communication. Cameras provided a resolution of 640 ├Ś 480, and a maximum of 30 video frames per second. The lowest specifications of the computers used for conferencing were Pentium IV 2.0 CPUs and 512 MB RAM. The operating system used was Microsoft Windows XP. Minimum network speed was 100 kbps.
4. Hardware Setup
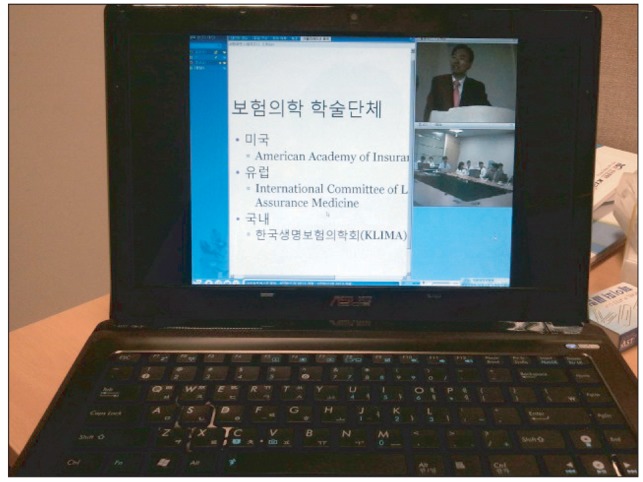
Two computers, two video cameras, three microphones, and one echocanceler were set up in a SNUHFM conference room, where most of the presentations were held. SNUBHFM set up a portable system that consisted of one laptop, one video camera, one microphone, and one echocanceler because SNUBHFM does not have its own conference room. A desktop computer installed in each conference rooms was used to project the presentation onto a large screen, and audio and video equipments were connected to a laptop to relay images and sounds. Installation of a mobile system could be completed in about five minutes, making participation in videoconferences possible anywhere with an internet connection. KNUHFM participated in videoconferences via a desktop computer. When necessary, members of KNUHFM could communicate with the other locations through a messenger window provided by the V2 Conference software.
Individuals who were unable to physically come to the conference rooms could participate in videoconferences on their own laptops at any location with an internet connection. With the presenters's permission, videoconferences were recorded as video files and uploaded to an internet materials room for later download and replay.
RESULTS
1. Videoconferences
Conferences are an important part of education in family medicine, and most hospitals hold conferences that include discussions of articles or textbooks and presentations on clinical themes.4) However, hospitals with a small numbers of staff members or residents have difficulties preparing independent conferences when their residents are dispatched to other departments or subsidiary hospitals.3) Even when human resources are sufficient, it is still difficult to maintain a high level of participation in conferences if residents are frequently dispatched to other departments or hospitals. Such factors negatively impact the quality of continuing medical education.2) In 2007, there were 104 hospitals with family medicine residency training programs in Korea. 60% of them were secondary hospitals, and 34 hospitals had only one family medicine staff member, while 30 hospitals had two staff members.6) According to a study conducted in 2003, 24% of family medicine residency training programs in Korea had one or two family medicine residents, and 33% had three to six residents.4) Joint videoconferences between hospitals through videoconferencing technology could be a solution to this problem. Speakers and audience in various geographic locations are able to exchange multimedia information, such as sounds, images and data, in real time through avideoconferencing system. Such systems may overcome time and spatial limitations and expand the range of education available.7) The quality and satisfaction rates of education through videoconferences are comparable to those obtained with conventional conferences.1,8,9)
Two small departments of family medicine (SNUBHFM, KNUHFM) that lack resources shared 81 joint videoconferences with SNUHFM, which has sufficient human resources, over a period of seven months through a videoconferencing system. After this period, we asked the members of SNUBHFM and KNUHFM about their satisfaction with the system. Most of the staff members and residents of SNUBHFM and KNUHFM were satisfied with joint videoconferences. All of them agreed that this system was helpful not only for the residents but also for the staff members in obtaining the latest knowledge in various areas. Residents were able to learn and receive feedback from residents and staff members of other hospitals. Because of these results, joint videoconferencing has been sustained between three hospitals.
Despite these positive results, it is undesirable to depend entirely on joint videoconferencing since each hospital has unique issues and cases that might require more specific medical education. KNUHFM has added joint videoconferences to its own conferences which include topic review on Wednesday during lunchtime, case conferences on Tuesday and Friday afternoons, and journal review, book reading and obesity and anti-smoking education on Tuesday afternoons. Some improvements also need to be made to enhance the conferences, including the quality of the audio system, the stability of the videoconferencing system and the frequency of active discussions among hospitals.
2. Equipment Issues
General web cameras are sufficient for small-scale conferences in which two or three people participate and watch the presentation on a computer screen. However, web cameras are not appropriate for large-scale conferences in which more than ten people participate and speakers make presentations from a podium. Cameras used for large conferences should be remotely controllable, rotate 180 degrees, have high resolution, move up and down 90 degrees, and be freely zoomed in and out to transfer a realistic conference atmosphere to remote locations. Cameras that we used for joint videoconferences fulfilled these requirements.
The audio system is an important element in videoconferencing. Slight decreases in the quality of the image did not cause major inconvenience, but low sound quality led to communication difficulties and decreased concentration on the videoconference. Personal headsets or general speakers connected to computers are good enough for small-scale video conferences. However, because general speakers and microphones can produce howling and echo effects, which degrade the quality of the videoconference, they are not appropriate for large-scale conferences in which many participants may speak freely at once. Therefore, an echocanceler that eliminates echo effects and howling should be used for larger conferences. Generally, echocancelers for videoconferences are expensive, costing more than 1 million Korean won. We made an effort to build an affordable, cost effective conference model. After researching our options, we decided that we could purchase an echocanceler (XING) at 240,000 Korean won.
In conclusion, joint videoconferencing between multiple family medicine departments is feasible, satisfactory and useful for continuing medical education, especially when the participating family medicine departments lack the resources to hold regular conferences on their own. We expect that more family medicine departments will participate in implementing such joint videoconference systems in the future.