INTRODUCTION
Telemedicine is the application of telemetry in the practice of medicine. It has many definitions, from a simple one involving a provision of medical information and services using telecommunication and information technology, to a more comprehensive definition as in usage of exchanged medical information through electronic networks to improve a patient's education, healthcare provider's education, and patient care.1)
The beginnings of telemedicine are unclear. What we do know is that the Nebraska Psychiatric Institute was one of the first facilities to use closed-circuit television for healthcare purposes, while moving away from simpler forms of communicating. Some of the early forms of telemedicine included advice to patients living in remote areas and requiring medical care, by using a telephone or a radiotelegraph in 1959.2) Thereafter, telemedicine made rapid progress together with the development of information and communication technology. These improved a patient's welfare by providing appropriate medical services to a vulnerable class of people who were unable to receive appropriate medical treatment either because of war and/or regional problems.
As an example, telemedicine contributed to the reduction of sudden accidents to under 3% during the Gulf War in 1991.2) In Korea, telemedicine began as a demonstration project in teleradiology between Seoul National University Hospital and Yeoncheon Health Center in 1988. Thereafter, a demonstration project was conducted for the vulnerable class in tertiary hospital and this gradually expanded the range of medical services.
A 2005 study was conducted among chronic disease patients using a remote management service in Gangwon-do. Findings were encouraging: on a scale of 1 to 5, with 5 displaying the most positive traits, satisfaction was 4.07, accessibility was 3.95, and usefulness was 4.15.3) In addition, results from the ministry of health and welfare's project evaluation regarding u-health demonstration projects conducted in 2003 also contributed to an improvement of convenience in using medical services.
Compared with the existing face-to-face patient care, telemedicine can help to reduce round trip time to a medical institute, transportation expenses, and opportunity cost.4)
When telemedicine is implemented, it provides not only a positive benefit to medical patients who are vulnerable, but also a time and economic benefit to general primary care users, especially patients with chronic diseases. Telemedicine is a common practice pattern among family physicians wishing to make the first contact with a patient. This study was designed to investigate the patient's knowledge and preferences toward telemedicine and provide family physician with information to help establish a proper practice plan and direction.
METHODS
1. Study Participants
This study was conducted in family medicine clinics and health promotion centers of a university hospital in Seoul metrocity and Chungju city from April 1, 2010 to May 31, 2010. Subjects included 275 participants who were older than 18 years and had agreed to take part in the study. Of these, 32 participants with incomplete responses were excluded. Thus, the current study consisted of a total of 243 respondents.
2. Questionnaires
The questionnaire consisted of the following 21 items: socio-demographic characteristics, knowledge and preference towards telemedicine, preferred department to get treated for a disease, ideal range of medical services and healthcare institution about telemedicine, and appropriate costs in comparison with face-to-face patient care. The participants were also asked to provide reasons for preferences and non-preferences.
3. Statistical Analysis
The characteristics of the study participants and attitudes toward telemedicine were analyzed using descriptive statistics. χ2-test and trend test were employed for analysis of relevant factors on awareness and preferences toward telemedicine. We also used a Fisher's exact test if the sample size was 5 or less. Statistical analysis was performed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). A significance level of 0.05 was set for all tests.
RESULTS
1. Characteristics of Study Participants
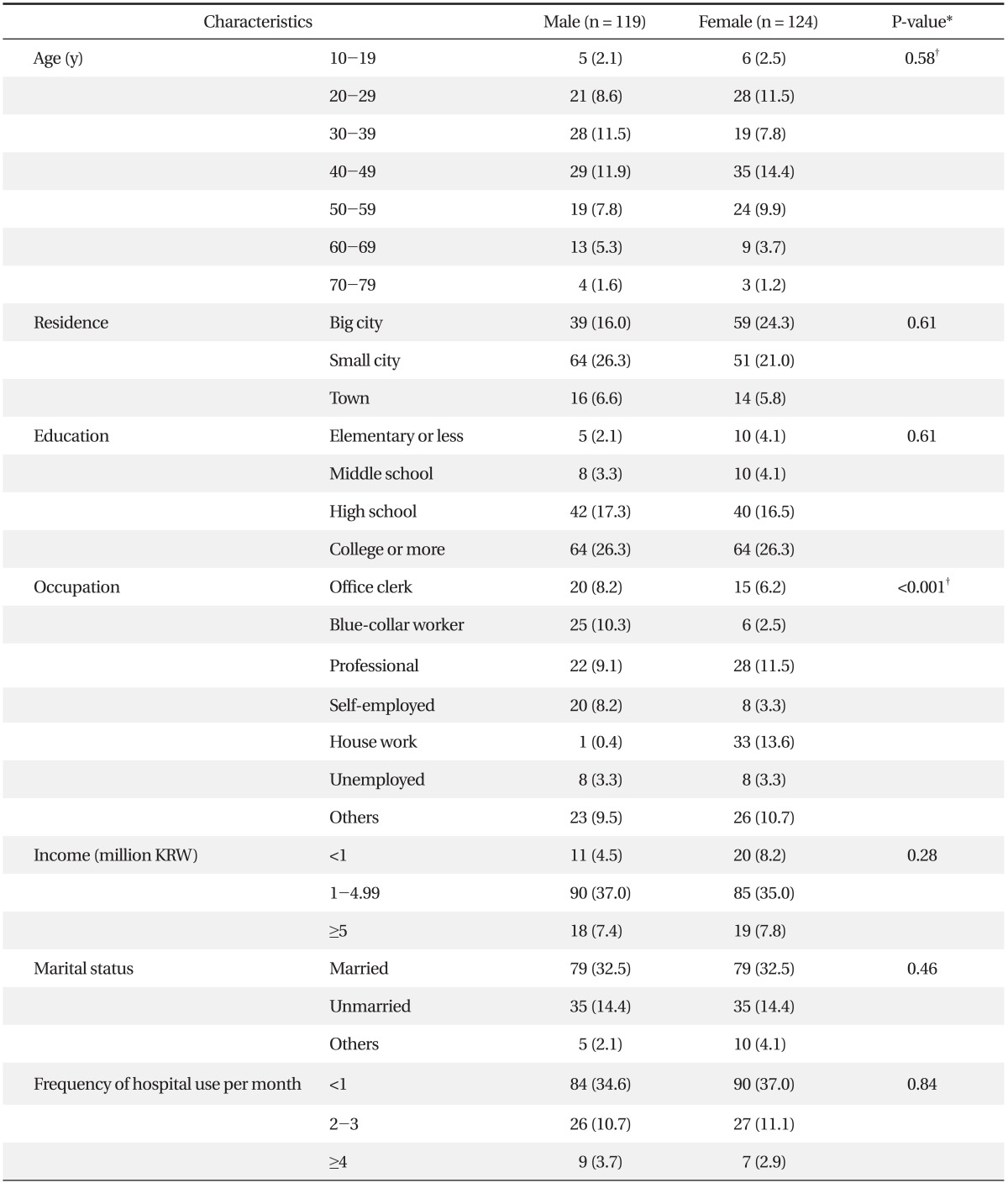
The baseline characteristics of the study participants are shown in Table 1. Of the 243 participants, 119 (49.0%) were males and 124 (51.0%) were females. City size residences of participants were small city (47.3%), big city (40.3%), and town (12.3%). The largest age group was 40-49 years (26.3%). Mean age of the participants was 41.85 (± 14.04) years. Level of education ranged from elementary or less (2.1%) to college or more (52.7%). Monthly incomes ranged from less than 1 million Korean won (12.8%), 1-4.99 million Korean won (72.0%), to more than 5 million Korean won (15.2%). Participants with professional jobs comprised the largest group (20.6%).
2. Awareness of Telemedicine
Awareness of telemedicine was 49.8% and there was a significant difference in resident area, educational level, and occupation. Participants living in towns (36.7%) were the least aware, followed by those living in a small city (44.3%), and finally those living in a big city (60.2%; P = 0.007). There was a significant difference in awareness according to education (P = 0.03), but the trend according to education was not. There was a significant difference in awareness based on occupation (P = 0.02). Information of telemedicine was obtained via television (44.4%), hospital (19.7%), and the internet (16.2%) (Table 2).
3. Preference towards Telemedicine
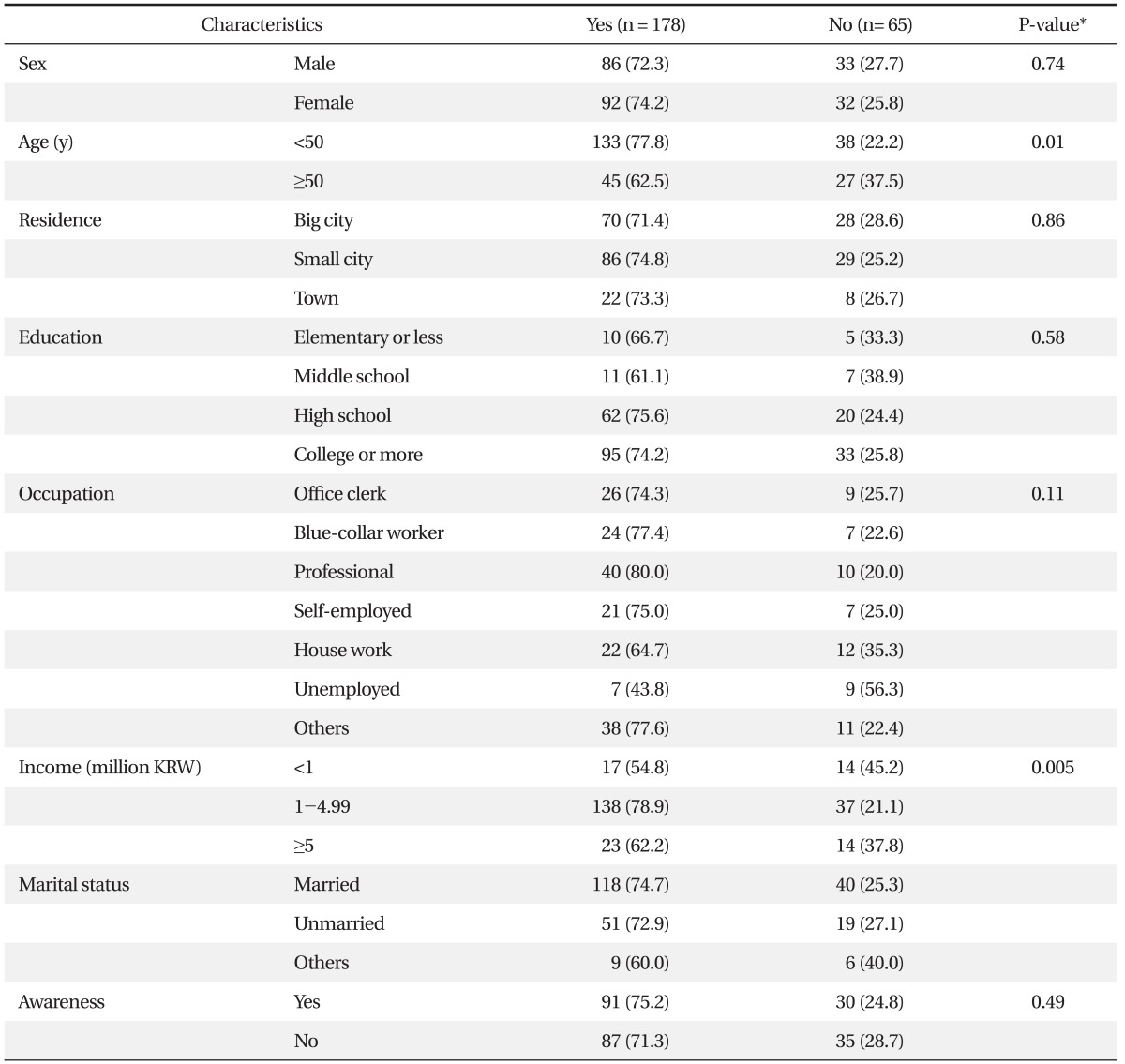
A majority of participants prefer telemedicine (73.3%). Younger participants (those aged below 50 years) were more likely to prefer than older participants (those aged more than 50 years) (P = 0.01). Differences in participant preferences also revealed differences according to income levels: 1-4.99 million Korean won (78.9%), more than 5 million Korean won (62.2%) and less than 1 million Korean won (54.8%; P = 0.005) (Table 3).
4. Reasons for Preference and Non-Preference
The reasons for preference were convenience (85.4%), rapidity (53.4%), and accessibility (27.8%). The reasons for non-preference were lower reliability (49.2%), lower quality (40.0%), and difficulty of using equipment (18.2%). In particular, those aged less than 50 years showed a greater preference for telemedicine because of convenience and accessibility (P = 0.031 and P = 0.003, respectively). Participants with higher education, convenience, and accessibility tended to choose high preference reasons (P = 0.002 and P = 0.002, respectively). Among those living in more urbanized areas, convenience was the reason for preference (P = 0.001). Participants with higher monthly incomes chose accessibility as a preference reason (P = 0.004) (Table 4). Among the reasons for participants who did not prefer telemedicine, there was no difference in age for reliability, those who were below 50 years chose lower quality (P = 0.001), and those who were more than 50 years chose difficulty of using equipment (P = 0.002) (Table 5).
5. Other Characteristics of Telemedicine
1) Appropriate cost of telemedicine
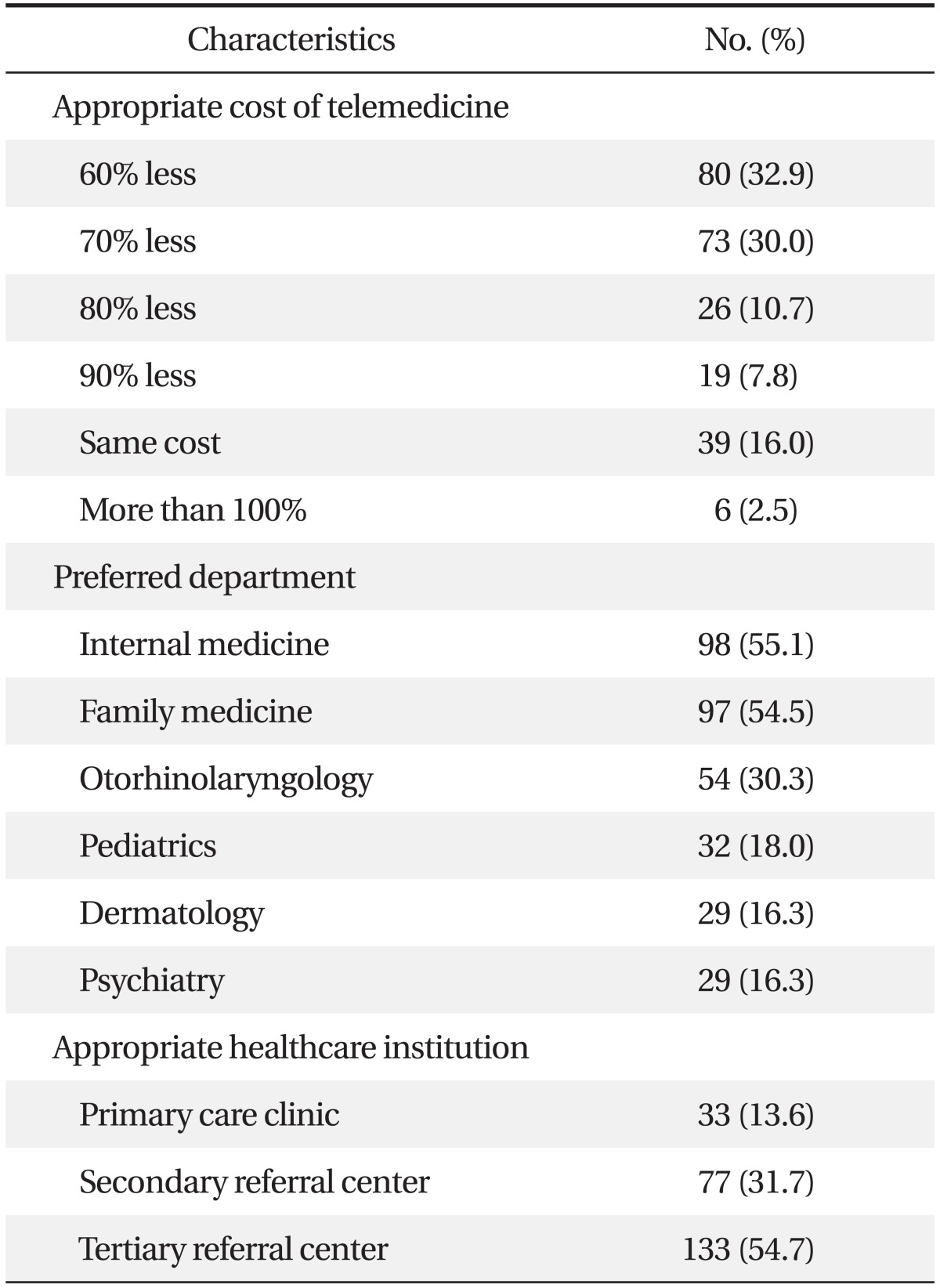
Compared to face-to-face patient care costs, the cost of telemedicine ranged from 60% less (32.9%), 70% less (30.0%), the same (16.0%), and more than 100% (2.5%). A majority of participants regarded lower than face-to-face patient care cost as proper (Table 6).
2) Preferred department
When participants were permitted multiple selections about their intention to get treatment, participants chose internal medicine (55.1%), family medicine (54.5%), otorhinolaryngology (30.3%), pediatrics (18.0%), dermatology (16.3%), and neurology (16.3%) as the most likely medical fields to receive treatment.
3) Appropriate healthcare institution
Participants chose tertiary referral center (54.7%), secondary referral center (31.7%), and primary care clinic (13.6%) as appropriate health institutions for telemedicine (Table 6).
DISCUSSION
"Health for All" is a programming goal of the World Health Organization, which envisions securing the health and well-being of people around the world. In Korea, the new health plan established in 2005 set a goal to expand life expectancy and secure health equity.5) Along with advancement in information and communication technology, universal accessibility in medical care service has gained great importance. These factors have led to an introduction of telemedicine in demonstration projects found within developed countries, including Korea.4,6) From demonstration project, they were able to assess that telemedicine can offer both economic and time saving benefits to medical consumers, and provide them with great satisfaction.1) Since telemedicine in Korea is still at an early stage, in order for it to become a universal service, much time and effort will be needed to establish policy directions and social agreements.1,7-9) At the same time, we believe that telemedicine will eventually become an important part of Korea's medical services.
In this study, awareness of telemedicine was 49.8%, a fairly low figure, which is almost similar to findings by Lee et al.10) This awareness differed depending on where the person lived, his/her education level, and his/her occupation. Awareness was greatest among those who live in big cities, but decreased when residence moved from small cities to towns. This difference was seen by education level, but it was not statistically significant. As explained by Chang et al.11) the difference is due to the health information approach being diverse, depending on the consumers' characteristics. The Korea Health Industry Development Institute consumer survey in 200812) reported that a major cause for the inhibition of activating and systemizing u-heath is due to a lack of u-healthcare-related promotion and education (31.7%), but our study showed that there was no association between awareness and preference.
There was a preference difference in telemedicine at 50 years of age. Those who were 50 years and older had major difficulties in manipulating the instrument. This may be explained by the "techno-terror" that those over 50 years old encounter.2) However, Kim et al.13) have shown that even though skilled techniques may decrease among the elderly, when asked to manipulate the u-health instrument during the study, the elderly had a higher set of skills compared to younger first-time users. When the elderly are given a thorough and sufficient education, this so-called "techno-terror" may not seem as problematic as once thought.
Since the chronic disease patients are more concentrated in the tertiary hospitals, the medical costs for these patients are much higher compared to the general hospitals or local clinics. As the medical needs are greatest for those at 60 years and older,14) cost-effectiveness may be poor. By relieving the fear in using telemedicine services among the elderly, an efficient medical service may be provided. Monthly incomes that were lower than 1,000,000 won had the lowest preference in telemedicine. As income increased, preference for telemedicine also rose. This finding suggests that those with higher income are more likely to use telemedicine services, consistent with previous results.15) Thus, by increasing the preference of telemedicine in the low-income population, and thereby raising its use as a health care method, cost reductions may occur.
Participants younger than 50 years had other reasons for non-preference, involving concerns for less reliability and poor quality of medical care services. Many studies have shown that the telemedicine care group had a more efficient medical care service than the control group,14,16,17) and thus, the issue of low reliability and quality may be unwarranted. When asked what was considered an adequate cost for the telemedicine medical care, a majority of respondents preferred 60% to 70% off a face-to-face care cost. However, according to Koh and Cho15) a study conducted on chronic disease patients living in a rural area in Korea revealed their willingness to pay higher costs for community health care service than for telemedicine. This suggests that from the consumers' point of view, telemedicine care has a higher monetary cost. The difference in study findings may have resulted from a difference in study population; our sample was based on university hospital patients who never experienced telemedicine care service.
When asked for a preference of department for which they wished to be served in telemedicine, internal medicine was the most preferable, followed by, family medicine, otolaryngology, and pediatrics. When asked for an appropriate medical facility for the telemedicine, tertiary hospital was chosen as most appropriate, followed by, secondary and primary. However, when considering cost-effectiveness and a need for re-establishing a collapsed health care delivery system, telemedicine should be mobilized from primary care settings.2) Thus, it would make sense for the present telemedicine promotion project performed in tertiary hospitals to liaison with primary care clinics.
This study was designed to investigate the patient's knowledge and preference towards telemedicine and provide the family physician with information to establish a practical plan and direction. However, there are several limitations.
First, even though this study sampled primary care patients who visited family medicine clinics, there was a lack of representativeness among primary care patients since these participants were recruited from a university hospital, which may have biased the results. Second, participants over 60 years of age, considered a vulnerable group of patients, had the lowest response to the questionnaires, which limited the understanding of awareness and preferences among people with the greatest needs for medical services. Third, the evaluation for awareness and preference was answered in a "yes or no" format, which limited its interpretations when translating to real attitudes.
Telemedicine has been possible following the advancement of information technology. At present, telemedicine is only available to patients who are considered vulnerable. However, with an increasing need, the government will gradually expand its range and services. In order to provide telemedicine to all medical consumers, some issues will need to be addressed. First, new plans to improve Korea's legislations on telemedicine needs to be considered with u-healthcare-related support from the government, and social agreement from interest groups.
Secondly, in order to achieve a successful family-oriented telemedicine, easy access to operate the program and a capability to pursue health education by oneself is needed. Third, patient confidentiality should not be disclosed to others unless the individual has given specific permission for such release.7,9,14) Fourth, as mentioned earlier, there needs to have sufficient plans to solve uncertainties in the quality of telemedicine. Last, but not least, a sensible and adequate amount of telemedicine medical expenses should be settled.