INTRODUCTION
The common cold is one of the most common diseases occurring among all age groups and is the primary cause of visits to doctors in developed countries. According to The National Institute of Allergy and Infectious Disease,1) one billion common colds occur annually in the US and the average adult contracts two to four colds and children contract six to ten colds annually in the US. The socioeconomic cost of the common cold can be quite high ($5 billion per year in the US),2) as it is the one of the most common causes of absenteeism from work and school. Viruses are the most common cause of colds. The most causative virus is the rhinovirus, which accounts for 40% of colds. Thus, the term 'common cold' does not refer to a single entity but to a group of diseases caused by numerous unrelated ethological agents,3) so there is no specific treatment for the common cold besides symptomatic treatments. Therefore, prevention is the primary focus in managing the common cold. Hand-washing is the most effective and well-known preventive methods. A meta-analysis regarding the effects of probiotics on the prevention of the common cold4) showed that probiotics may have a preventive effect against the common cold. In addition, a recent Cochrane review reported that routine vitamin C supplementation did not reduce the incidence of colds in the general population but that it may be useful for people exposed to brief periods of severe physical exercise.3)
Some studies revealed that regular, moderate-intensity exercise affects the concentration of various cells impacting the body's immune system, especially immunoglobulin A (IgA) and natural killer (NK) cells.5) In a randomized trial about the effects of moderate-intensity exercise on immune response,6) 45 minutes of moderate-intensity brisk walking for 15 weeks was not associated with an improvement in lymphocyte function but was associated with a 20% increase in serum immunoglobulin including IgA, immunoglobulin M, and immunoglobulin G. Another study investigating the association between moderate-intensity exercise and upper respiratory tract infections (URTI)7) reported that exercise reduced the number of days subjects suffered from URTI and the severity of their symptoms.
However, there has been no systematic review or meta-analysis of the effects of exercise on prevention of the common cold. Therefore, this study investigated the effects of regular, moderate-intensity exercise on the prevention of the common cold through a meta-analysis of randomized controlled trials.
METHODS
A meta-analysis of randomized controlled trials was performed to investigate the effects of regular, moderate-intensity aerobic exercise on the prevention of the common cold in the general population.
1. Inclusion Criteria
The systematic review included randomized controlled trials comparing differences in the incidence rate of common colds between a regular, moderate-intensity aerobic exercise group and a control group with no exercise. Regular exercise was defined as exercise performed more than 5 times per weeks, and moderate-intensity was defined as greater than 60% of maximal heart rate. Studies about lower respiratory tract diseases, such as pneumonia, tracheitis, bronchitis; studies about URTI other than the common cold, such as tonsillitis or otitis media; and studies about specific diseases, such as diabetes or hypertension, were all excluded.
2. Search Methods
The final search was performed on June, 2013. All searches were performed by professional librarians. There was no language restriction.
The searches were made on MEDLINE (PubMed), EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), and CINAHL. The keywords for MEDLINE and EMBASE search were as follows.
-
#1 Colds, Common OR Common Colds OR Cold, Common OR Coryza, Acute OR Acute Coryza OR Catarrh OR Catarrhs OR Infection, Respiratory Tract OR Respiratory Tract Infection OR Respiratory Infections OR Infections, Respiratory
Infections, Respiratory Tract OR Upper Respiratory Tract Infections OR Infections, Upper Respiratory Tract OR Upper Respiratory Infections OR Infections, Upper Respiratory OR Respiratory Infection, Upper OR Rhinoviruses OR Coryza VirusesCoryza Virus OR Common Cold Virus OR Cold Virus, Common OR Cold Viruses, Common OR Common Cold Viruses -
#2 Exercises OR Exercise, Physical OR Exercises, Physical OR Physical Exercise
Physical Exercises OR Exercise, Isometric OR Exercises, Isometric OR Isometric Exercises OR Isometric Exercise OR Warm-Up Exercise OR Exercise, Warm-Up OR Exercises, Warm-Up OR Warm Up Exercise OR Warm-Up Exercises OR Exercise, Aerobic OR Aerobic Exercises OR Exercises, Aerobic OR Aerobic Exercise #3 Controlled Clinical Trials, Randomized OR Clinical Trials, Randomized OR Trials, Randomized Clinical
#4 #1 AND #2 AND #3
In addition, an additional search was performed on the reference listed in each of the included studies.
3. Study Selection
Two independent authors reviewed the search results and selected studies satisfying the inclusion criteria; any disagreements between two authors were settled by discussion and consensus. If the two authors were unable to reach an agreement, a final decision was made by the third author.
4. Assessment of Risk of Bias
Quality assessment of the selected studies was performed using the Cochrane Collaboration's tool for assessing risk of bias.8) Each item was classified as low risk, high risk, or unclear; low risk for low risk of bias, high risk for high risk of bias, and unclear for difficult to decide. The assessment was done by two independent authors, and any discrepancies between the two authors were resolved by discussion and consensus.
5. Data Extraction
Two independent authors independently carried out the data extraction using standard data extraction forms. Numbers and characteristics of participants, type and duration of exercise, control group details, follow-up period, and outcome variables were extracted. Discrepancies between two authors were resolved by discussion.
6. Statistical Analysis
Dichotomous data were presented as relative risk with 95% confidence intervals (CI), while continuous data were presented as mean difference. Review Manager ver. 5.2 (RevMan; Cochrane Collaboration, Oxford, UK)9) was used to analyze the study results. The results were summarized through a forest plot, and a funnel plot was planned to check for publication bias if a number of the studies were to be over 10. I2 is a form of statistics that quantifies inconsistency, and the I2 test was applied to identify heterogeneity as well. I2 ranges from 0% to 100%, and values between 0% and 40% were interpreted as unimportant heterogeneity, up to 60% as moderate heterogeneity, and over 60% as considerable heterogeneity. In the case of statistical homogeneity, a fixed-effects model was applied, whereas in the case of statistical heterogeneity, a random-effects model of meta-analysis was used. P-values lower than 0.05 were considered statistically significant. A subgroup analysis was conducted to evaluate the duration of exercise.
RESULTS
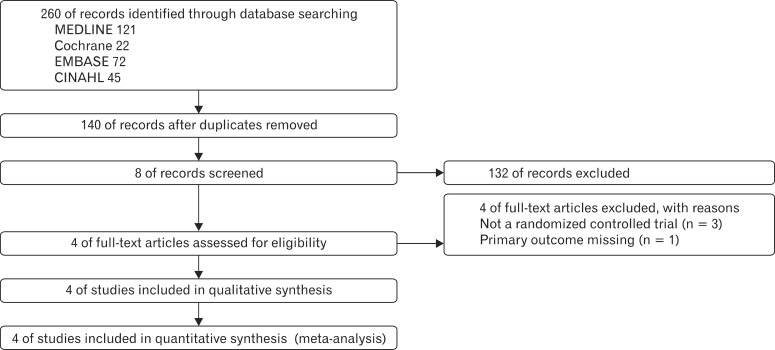
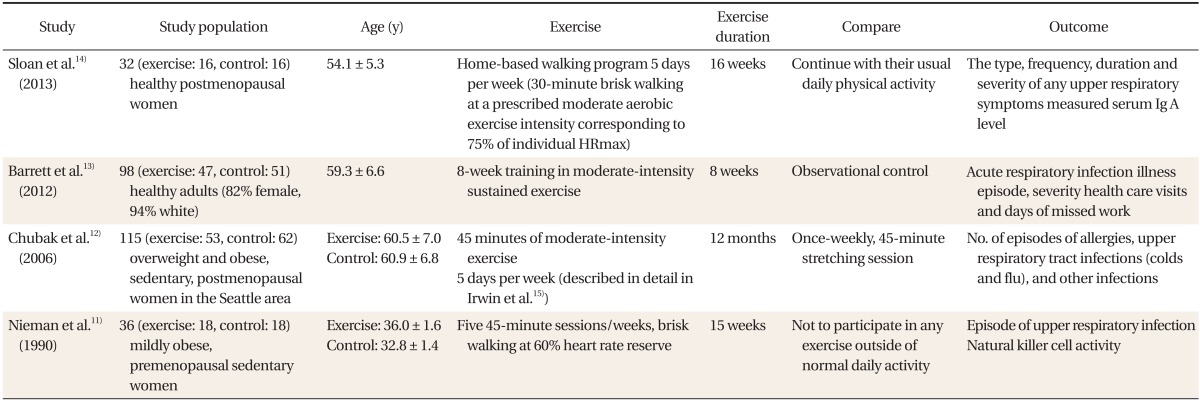
A total of 260 articles were retrieved from electronic searches including 121 articles from PubMed, 22 articles from Cochrane, 72 articles from EMBASE, and 45 articles from CINAHL. A total of 140 were screened and eight studies were found to be relevant to this study. Of these, five studies were selected during the full-text review process. One study10) did not have the sufficient statistical data regarding the incidence rate of colds in the participants. The author of this study was contacted by e-mail, but did not reply. Thus four randomized controlled trials11,12,13,14) were selected and included in the analysis (Figure 1). The characteristics of the included studies are shown in Table 1.15) Ultimately, only three studies11,13,14) out of four had sufficient data to extract the mean number of days participants were sick from the common cold.
A total of 281 participants were included; 134 participants were in the exercise group and 147 were in the control group. All studies were conducted in the US. One study12) referred to the seasons during which trial was conducted while the remaining three did not. In three studies all participants were female, while in one study13) 18% of participants were male. In one study11) all participants were in their 30s, while in the other three studies all participants were in their 50s or older. In all included studies, monitoring of incidence and duration of common colds was done during the trial period. None was tested for long term effects. Two of the four studies13) had measured the incidence and mean duration of upper respiratory infection during intervention period. In other study, participants were monitored two more months after intervention.
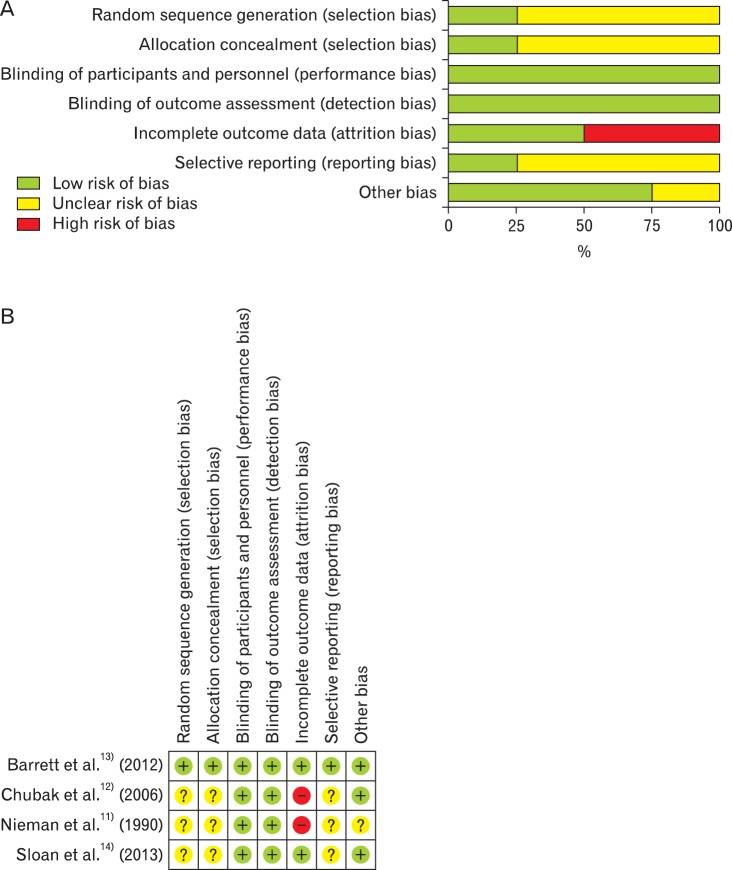
The risk of bias for the included studies was evaluated using the Cochrane Collaboration's tool for assessing risk of bias.8) It was evaluated that items for appropriate random sequence generation and allocation concealment were low-risk in one study,13) but deemed to be unclear in other three studies. Due to the nature of the studies, blinding of participants was not performed, though it was determined that the outcome was not likely to be influenced by a lack of blinding. Two studies11,12) showed a high risk of bias regarding incomplete outcome data reporting. One study13) showed a low risk of bias in selective reporting, and the others were unclear. Only one13) study was evaluated as a relatively high quality study; the other three studies did not provide enough data to assess the quality of the studies (Figure 2).
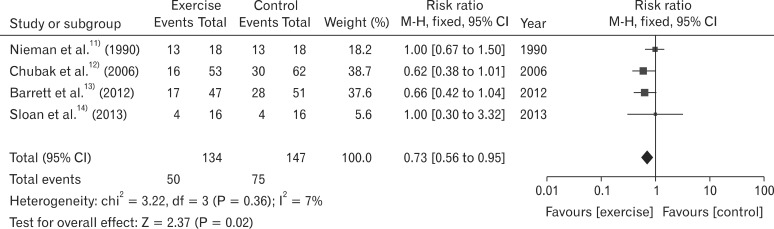
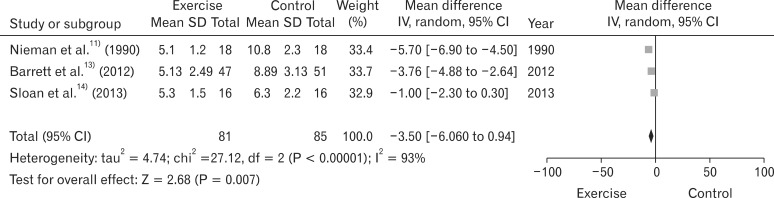
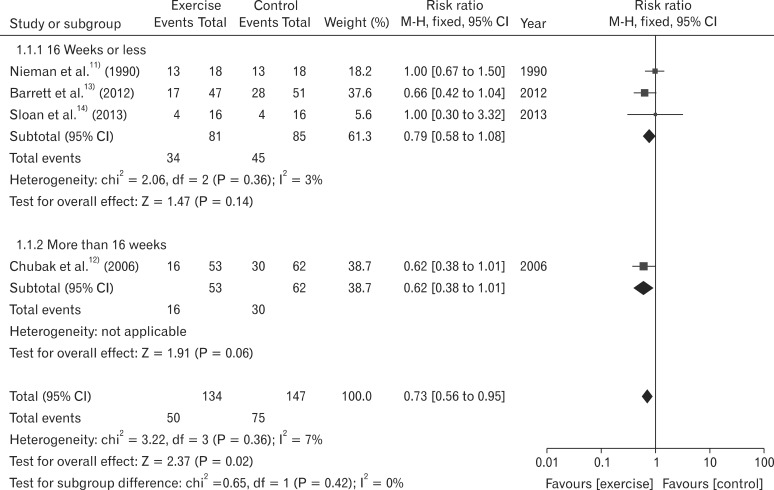
After analyzing all four studies, the relative risk of the common cold in exercise groups compared to the control group was 0.73 (95% CI, 0.56 to 0.95; I2 = 7%) (Figure 3). Three studies that reported mean illness days were analyzed as well. The mean difference between groups was -3.50 (95% CI, -6.06 to -0.94; I2 = 93%) (Figure 4). A subgroup analysis was conducted based on exercise duration. In the first subgroup with three studies11,13,14) that had participants exercising for 16 weeks or less, the relative risk was 0.79 (95% CI, 0.58 to 1.08; I2 = 3%), but there was no statistically significant difference. In the second subgroup with one other study that had participants exercising for more than 16 weeks, the relative risk was 0.62 (95% CI, 0.46 to 0.89) (Figure 5). Because the number of included studies was less than 10, a funnel plot was not produced.
DISCUSSION
According to this meta-analysis of four studies about the effect of exercise on the prevention of the common cold, the relative risk of the common cold in exercise groups compared to the control group was 0.73 (95% CI, 0.56 to 0.95; I2 = 7%). The incidence rate of the common cold declined significantly in the exercise group, and there was no heterogeneity between studies. To identify the effect of exercise on the severity of the common cold, mean illness days as outcome variables was analyzed. Three studies had data outcome regarding mean illness days, and the mean difference was -3.50 (95% CI, -6.06 to -0.94; I2 = 93%), with significant heterogeneity between studies.
In a subgroup analysis based on exercise duration, the relative risk of the subgroup with participants who exercised for 16 weeks or less was 0.79 (95% CI, 0.58 to 1.08; I2 = 3%), but there was no statistically significant difference between groups. There was only one study with participants who exercised for more than 16 weeks exercise, and thus a subgroup comparison was not relevant. Because only four studies were included in this meta-analysis, it was not possible to draw a meaningful conclusion as to how exercise duration may help to prevent the common cold.
Several mechanisms have been proposed to explain the relationship between moderate excise training and risk of URTI. Barrett et al.13) evaluated potential preventive effects of exercise on incidence, duration of URTI. They also analyzed interleukin-8, neutrophil count-biomarker of inflammation. But, between-group differences were not statistically significant for these biomarkers. A randomly controlled 15-week exercise training study was conducted to investigate the relationship between changes in NK cell number, activity, and URTI symptomatology. Nieman et al.11) founded that exercise training did have a significant effect on NK cell activity especially during the initial 6-week period. Another study demonstrated an inverse relationship between salivary IgA concentration and risk of URTI.14) From the results of these studies, the protective effects of regular, moderate-intensity aerobic exercise on colds may be partially explained by the immune status difference between the exercise group and control group. However the findings from these studies are inconsistent.16)
This study has several limitations. First, because only four studies met the inclusion criteria, there were limitations regarding power and homogeneity among studies. In addition, each study had a small sample size, so the total number of participants in the meta-analysis was also small. Furthermore, most of the participants were women. Therefore, the results may not be applicable to men. The quality of the studies also could not be evaluated precisely because the included studies did not provide enough data for an accurate quality assessment. It was not possible to analyze how time of year affects incidence of the common cold, as only one study mentioned the time of year during which the trial was conducted, and even in that study there were no data about seasonal incidence rates of the common cold. Participant age was not taken into consideration in this meta-analysis, even though age greatly influences incidence of the common cold. Of the four studies included in this final analysis, participants in three of the studies were all in their 50s or older, while participants in one study were all in their 30s. No children were included in this meta-analysis.
In conclusion, the effects of exercise on the common cold were investigated through a meta-analysis of randomized controlled trials. The results suggest that regular, moderate-intensity aerobic exercise may have preventive effects on colds. However, the number of included studies and participants was too small, the quality of selected studies was relatively poor, and there was insufficient analysis of variables that may impact incidence of the common cold. Therefore, there was not enough information to draw a clear conclusion from this meta-analysis. Subsequent well-designed, large randomized controlled trials are needed to clarify the association between exercise and incidence of the common cold.