INTRODUCTION
Physical activity refers to any bodily movement produced by the skeletal muscles that results in energy expenditure [1]. Physical activity improves musculoskeletal and mental health and reduces the risk of metabolic diseases, cardiovascular diseases, and cancer [2]. It improves cognitive ability in children and adolescents, lowers the risk of functional restriction after middle age, and extends healthy life expectancy [3]. However, a sedentary lifestyle is associated with adverse health outcomes, including metabolic disease, musculoskeletal disease, cancer, depression, and increased risk of cardiovascular and all-cause mortality through metabolic, hemodynamic, and neuro-hormone mechanisms [4]. Therefore, the importance of physical activity is emerging in modern societies, where major non-communicable diseases are increasing.
In the past, vigorous exercise was emphasized to obtain health benefits, but since the mid-1990s, moderate-intensity physical activity has been recommended because of its health benefits with less risk of injury [5]. The recent major guidelines regarding physical activity include the “Physical activity guidelines for Americans” published in 2018 and World Health Organization (WHO) guidelines published in 2020 [6,7]. According to these guidelines, all adults are encouraged to undertake 150–300 minutes of moderate-intensity physical activity or 75–150 minutes of vigorous-intensity physical activity or some equivalent combination of moderate-intensity and vigorous-intensity aerobic physical activity, per week, and to perform muscle-strengthening exercises on 2 or more days a week. Children and adolescents should perform 60 minutes or more of moderate-to-vigorous physical activity daily, including at least three days of vigorous-intensity aerobic physical activity and muscle-strengthening activity. Additionally, reducing sedentary behavior is recommended across all age groups [7].
Global age standardized prevalence of insufficient physical activity was 27.5% in 2016, with a difference between sexes of more than 8% points (23.4%, in men versus 31.7%, in women) [8]. Between 2001 and 2016, the levels of insufficient activity were stable (28.5%, in 2001; change not significant). This implies the need for active interventions to increase physical activity levels. To improve physical activity levels, it is essential to recognize the trend and current situation of physical activity. Therefore, we reviewed the current status of physical activity in South Korea and worldwide. In addition, strategies for improving physical activity are reviewed and discussed.
GLOBAL PHYSICAL ACTIVITY STATUS
According to WHO physical activity fact sheet in 2020 [9], more than a quarter (28% of adults aged 18 and over, 32% of women, 23% of men) of the world’s adult population (1.4 billion adults) were insufficiently active in 2016. This means that they do not meet the global recommendations of at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic physical activity per week. This was used as the definition of physical inactivity in this study. The physical inactivity level was approximately twice as high in high-income countries as in low-income countries. Globally, 81% of adolescents aged 11–17 years were insufficiently physically active in 2016. Adolescent girls were less active than adolescent boys, with 85% versus 78% not meeting WHO recommendations of at least 60 minutes of moderateto-vigorous physical activity per day. The level of physical activity among people has not improved globally since 2001. In high-income countries, insufficient physical activity has increased from 31.6% (2001) to 36.8% (2016).
1. The United States
According to the Centers for Disease Control and Prevention (CDC) report in January 2022 [10], adult physical inactivity prevalence exceeded 25% in all states in the United States, except four states. There was a significant difference in the level of physical activity according to race and ethnicity. Overall, Hispanic adults (32.1%) had the highest prevalence of physical inactivity, followed by non-Hispanic Black (30.0%), non-Hispanic American Indian/Alaska Native (29.1%), non-Hispanic White (23.0%), and non-Hispanic Asian adults (20.1%). In addition, the prevalence of physical inactivity differed by region. States in the south (27.5%) had the highest prevalence of physical inactivity, followed by the Midwest (25.2%), Northeast (24.7%), and West (21.0%).
In the case of US adolescents [11], as of 2016, the prevalence of physical inactivity was 72%, with 64.0% for boys and 80.5% for girls, indicating a significant lack of physical activity among girls. However, the overall tendency between 2001 and 2016, physical inactivity prevalence decreased among adolescents (70.9% to 64% in boys and 80.7% to 80.5% in girls), showing a slight improvement in physical activity level compared to adults.
2. South America
Previous studies have shown that South America’s rate of physical inactivity is known to reach approximately 31% [12], indicating that it was higher than the aforementioned average. According to the South American Physical Activity and Sedentary Behavior Network published in 2019 [13], the prevalence of more than 150 minutes of moderate-to-vigorous physical activity per week was 60.4% (Brazil) and 82.9% (Chile) among men and 49.4% (Ecuador) and 74.9% (Chile) among women, indicating significant differences between countries and sex.
Regarding sitting time, prevalence of more than 4 h/d was 78.0% (Peru) and 37.2% (Chile) among men, and between 79.5% (Peru) and 33.7% (Chile) among women. In Brazil, 12.4% of men and 16.9% of women reported more than 4 h/d in TV viewing.
3. Europe
The physical activity status of 27 European countries is well described in “2021 physical activity factsheets for the European Union (EU) member states in the WHO European region.” [14]. Among the representative EU countries, prevalence of sufficient physical activity in Belgium was 17.8% among adolescents and 64.1% among adults. Estimated prevalence of sufficient physical activity in adults was found to be 12.8% in Bulgaria, 19.5% in Croatia, 24.3% in Finland, 59.9% (55–74 years) and 64.8% (55–74 years) in France, 22.6% in Germany, 34.9% in Hungary, 48.0% (18–69 years) and 32.8% (≥64 years) in Italy; over 50% (55–65 years) and 41.9% (≥65 years) in Poland, 30.6% in Slovakia, and 60% (≥15 years) in Spain. There are significant differences in the prevalence of physical activity among countries. Overall, the prevalence of sufficient physical activity among the adolescents was very low.
4. Asia-Pacific Countries
1) Japan
According to a study by Tanaka et al. [15] in 2019 about 35.1% of Japanese adult men and 27.4% of adult women had sufficient physical activity as of 2016. The rate of physical activity satisfaction gradually increased compared to that in 1995. For adolescents, according to a study in 2018, although it included small number of participants, only approximately 10% of adolescents were performing appropriate levels of physical activity [16].
2) China
According to a study on physical activity levels in Chinese adults from 2000 to 2014, the rate of sufficient physical activity during leisure time increased slightly from 2000 (17.2%) to 2014 (22.8%), but it is still below expectations [17]. The annual rate of increase in sufficient physical activity is approximately 0.42%, showing a marked increase among adults under the age of 50 years, while the prevalence in the population over the age of 55 years tends to decrease to -0.05% per year.
According to a 2016 Physical Activity and Fitness in China-The Youth Study, the level of aerobic physical activity among Chinese children and adolescents does not satisfy the recommended level [18]. According to the study, only about 29.9% of 166 million school children met the recommended daily physical activity, and only three in 10 achieved an “excellent” or “good” fitness mark set by national physical fitness standards. The prevalence of sufficient physical activity was higher in boys (32%) than in girls (28%) and higher in urban regions than in rural regions. It was estimated that the higher the age, the lower was the level of physical activity.
3) Australia
According to the reports by the Australian Institute of Health and Welfare [19], approximately 2.5% of the total disease burden in 2015 was due to physical inactivity. In 2017–2018, it was observed that 55% of the Australian adult population was insufficiently active, and women (59%) had a higher rate of inactivity than men (50%). The rate of insufficient physical activity generally increased with age. Among individuals aged 18–24 years, 41% of men and 48% of women were insufficiently active. Among those aged 65 and over, 69% of men and 75% of women were insufficiently active. Moreover, 23% of adults aged 18 and over met the muscle strengthening guidelines (22% of women and 25% of men). Only 15% of adults met both the physical activity and muscle strengthening guidelines—17% of men and 14% of women. Among adolescents aged 15–17, 84.2% of boys and 94.7% of girls did not meet the physical activity guidelines. Additionally, 77.8% of boys and 90.9% of girls did not perform sufficient muscle strengthening activities.
STATUS OF PHYSICAL ACTIVITY IN KOREA
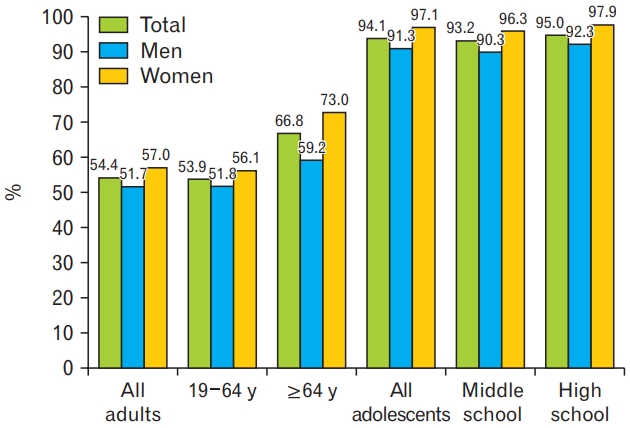
According to Korea National Health and Nutrition Examination Survey (KNHANES) reports and Korean Youth Health Risk Behavior Web-Based Survey (KYRBS) in 2020, the prevalence of insufficient physical activity was 54.4% in adults and 94.1% in adolescents, exceeding the global physical inactivity level aforementioned (28% in adults and 81% in adolescents, 2016) (Figure 1) [20,21]. The insufficient physical activity prevalence was higher in the elderly (≥65 years) than in young adults (18–64 years) and higher in women than in men (57.0% of women versus 51.7% of men). The difference in levels of physical activity according to sex was also observed in adolescents (97.1% of girls versus 91.3% of boys).
1. Status and Trends of Physical Activity in the Adults
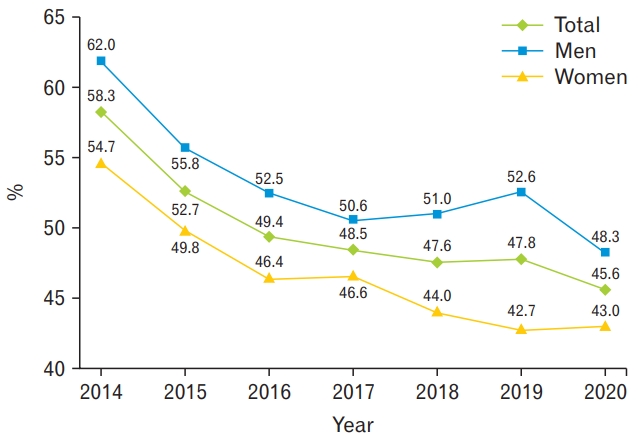
The KNHANES used the modified International Physical Activity Questionnaire Short Form until 2013. Since the Korean version of the Global Physical Activity Questionnaire was used in 2014, it was impossible to compare physical activity directly before and after 2014. There was continuous decrease in the prevalence of meeting the aerobic physical activity guidelines among Korean adults, from 58.3% in 2014 to 45.6% in 2020 (Figure 2) [20].
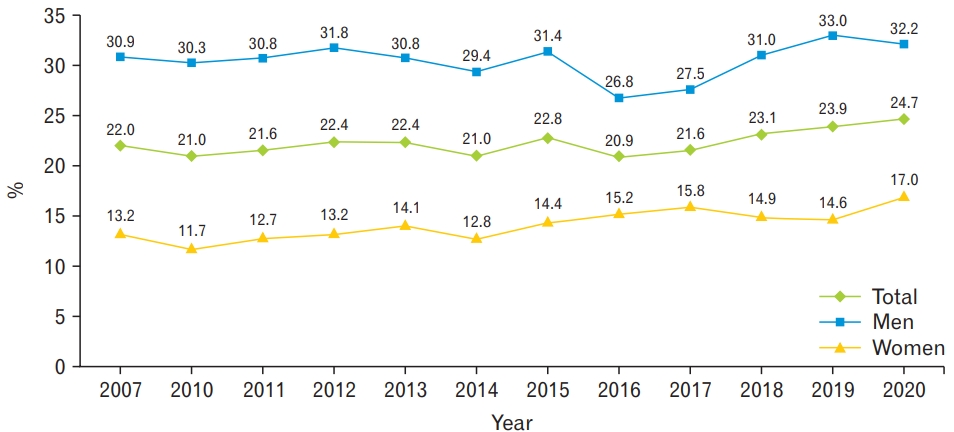
In the KNHANES, regular walking was defined as walking for more than 30 minutes at a time and more than 5 times per week, regardless of indoor or outdoor walking. Looking at the long-term trend since 2005, the rate of regular walking has decreased compared to the past, and currently, only about 40% of Korean adults practice regular walking (Figure 3)[20]. In terms of muscle-strengthening activity, only 24.7% of total adults perform muscle-strengthening activities at least 2 days per week, and there has been no significant change in the last decade (Figure 4) [20].
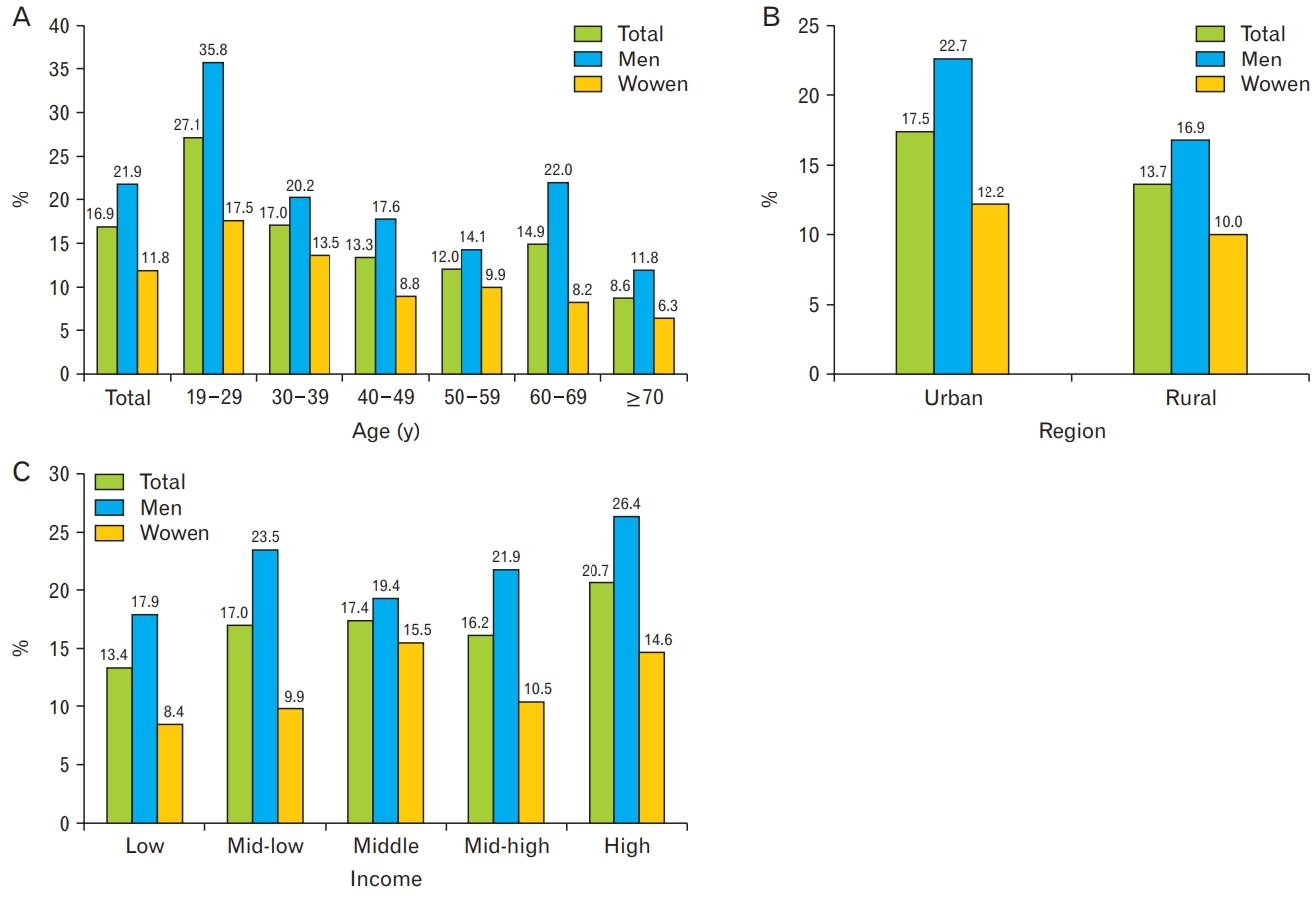
Only 16.9% of adults met both the aerobic and muscle-strengthening physical activity guidelines, and there was a significant difference (almost double) between men and women (21.9% versus 11.8%) (Figure 5) [20]. When classified according to age group, the prevalence was highest among those aged 19–29 years, and lowest among those aged 70 years and older. There were regional differences in the prevalence of meeting both the aerobic and muscle-strengthening physical activities, with 17.5% in urban areas and 13.7% in rural areas. The relationship between household income and the level of physical activity was not linear. However, both men and women had the lowest rate of aerobic and muscle-strengthening physical activity in the lowest income quintile and the highest rate of activity in the highest income quintile.
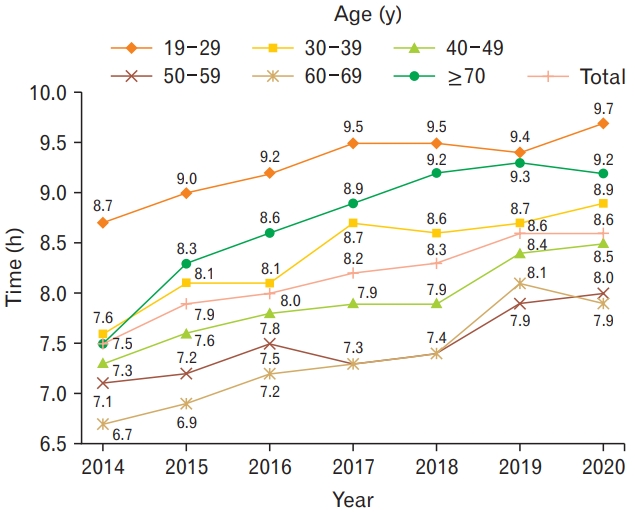
It is important to observe sedentary time as it is an independent risk factor for health. The sedentary time per day increased continuously from 2014 to 2020, and the results of the 2020 survey showed that approximately 8.6 hours per day were spent sitting among Korean adults (Figure 6) [20]. Sedentary time was longest among individuals aged 19–29 years (9.7 hours per day), and shortest among individuals aged 60–69 years (7.9 hours per day).
2. Status of Physical Activity in the Adolescents
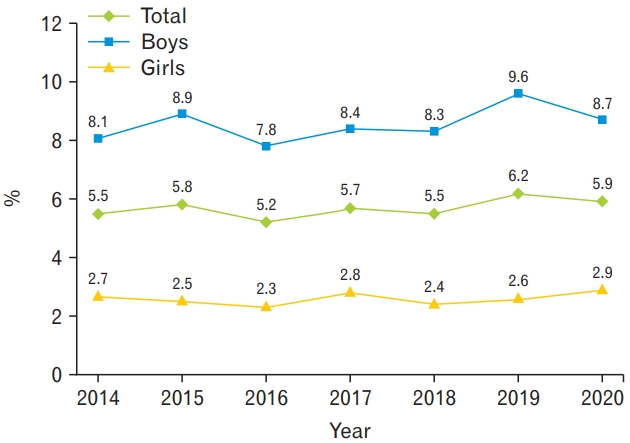
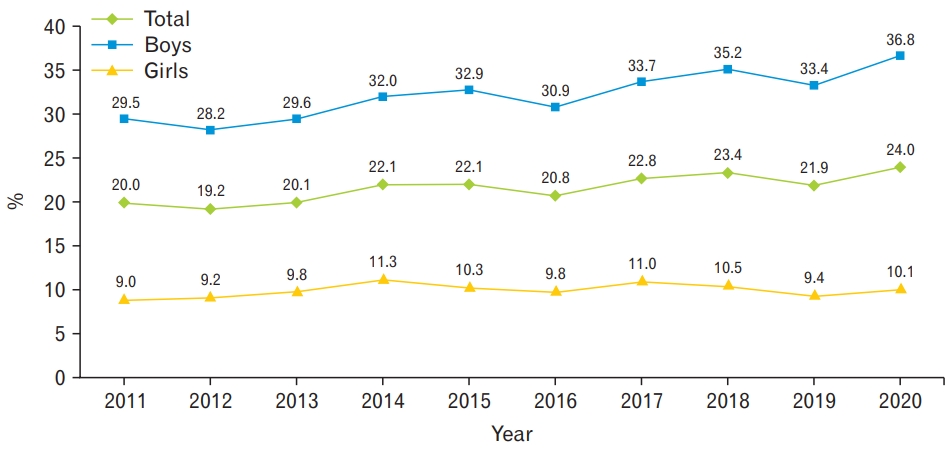
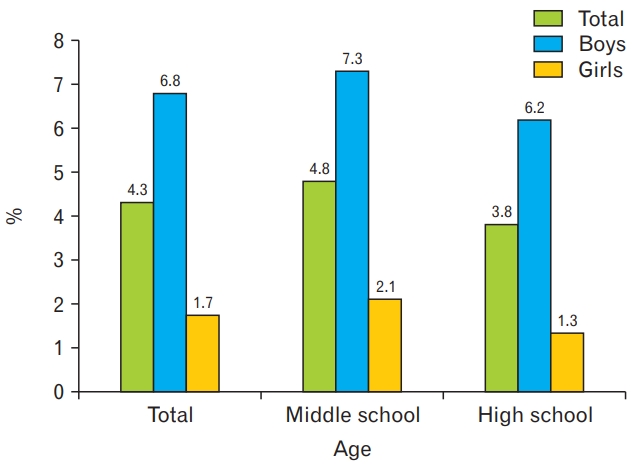
According to KYRBS 2020, only 5.9% of adolescents met the aerobic exercise guidelines, and the difference between the sexes was about three-fold: 8.7% for boys and 2.9% for girls (Figure 7) [21]. Only 24% of the total adolescents (36.8% of boys and 10.1% of girls) performed musclestrengthening activities in accordance with the guidelines (Figure 8) [21]. The prevalence of Korean adolescents who met both the aerobic and muscle-strengthening physical activity guidelines was 4.3%. There was significant sex difference (6.8% in boys and 1.7% in girls). The prevalence was lower among high school students than among middle school students (Figure 9) [21].
The daily sedentary time of adolescents is continuously increasing, and the 2020 data revealed that they spend an average of more than 10 hours a day sitting down (Figure 10) [21]. It was higher in girls than in boys (10.7 hours versus 9.9 hours), but the trend of sedentary time increased rapidly in boys over the past 3 years.
FACTORS RELATED TO PHYSICAL ACTIVITY
In Korea, the level of physical activity is low, and this phenomenon is becoming more serious. Determining the factors related to physical activity is essential to promote physical activity. According to previous studies, there are many factors related to physical activity, such as individual, interpersonal, environmental, regional or national policy, and global factors [22]. These can be largely divided into individual and environmental factors, and policy implementation is important to encourage physical activity. These three factors are described below.
1. Individual Correlates
Individual correlates included biological, demographic, psychological, and social factors. As for biological and demographic factors, age, sex, health status, educational level, and socioeconomic status could affect the level of physical activity. According to previous studies, physical activity is performed less often by old individuals, women, individuals with low socioeconomic level, and individuals with poor physical and/or mental health conditions [23]. Psychological factors include cognition, emotion, intention to exercise, outcome expectations, and self-efficacy. In particular, self-efficacy is conceptualized as a control belief referring to confidence in one’s ability to conduct the behaviors needed to reach a desired outcome, and many studies have revealed that it is a consistent and obvious personal factor that determines physical activity [24]. Social factors include support from home, friends, and work, and social support has a favorable effect on health-related behavior. Meanwhile, studies have shown that appropriate incentives increase physical activity performance [25,26].
2. Environmental Correlates
Environmental factors affecting physical activity can be classified into facilities, neighborhood, and social environmental factors. The effect of accessibility as a facility-related factor is well known, and a study based on the Community Health Survey has also reported that high accessibility to exercise facilities increases the degree of physical activity. [27]. Neighborhood factors, including parks, footpaths or bicycle paths, location of buildings, and community design, can affect physical activity. Regarding social and environmental factors, safety and transportation are relevant variables [22].
3. Policy Correlates
There are not much prior data that directly studied the influence of policy; however, recent studies describing global trends show that there is a wide variation in the level of physical activity according to regions and countries, suggesting that many factors influencing physical activity are at national and community levels [8]. Policies can affect the overall population for a long period of time. Policies can affect physical activity at the local (school or workplace), local government, or national level [28], and policies enable investment in resources or develop public health regulations [29]. More than 70% of countries currently operate physical activity-related policies; however, their scale and effectiveness are still insufficient to facilitate actual physical activity levels [8]. A study demonstrated that policy implementation yielded effective results in schools and infrastructure sectors, but insufficient results in economic sectors [30]. In a cross-sectional study that included 76 countries, the effectiveness of physical activity policies was low to moderate [31]. However, there were successful examples of promoting physical activity on a national scale presented from Finland, Canada, Brazil, and Colombia [32].
CURRENT STATUS OF PHYSICAL ACTIVITY POLICIES IN COUNTRIES AROUND THE WORLD
1. WHO Global Action Plan on Physical Activity 2018–2030
WHO has developed a global action plan to provide a framework for effective and feasible policy actions for countries to increase physical activity levels [1]. The target of this recent action plan includes a 10% relative reduction in the global prevalence of physical inactivity by 2025 and 15% reduction by 2030. To accomplish this, WHO provided four strategic objectives and 20 multidimensional policy actions. The four strategic objectives are as follows: (1) creating active societies in terms of social norms and attitudes; (2) creating active environments, including safe spaces and places for regular physical activity; (3) creating active people, providing programmers and opportunities, and promoting access, and (4) creating active systems, including governance and policy enablers, to promote physical activity and reduce sedentary behavior. The guideline presents 20 action plans comprising four to six plans related to each goal.
2. The United States: Active People, Healthy Nation: Creating an Active America, Together
Under the leadership of the CDC, the United States is working on an “Active People, Healthy Nation” program to promote physical activity [33]. The initiative aims to improve physical activity for about 27 million Americans by 2027, to allow 15 million people who do little aerobic exercise to begin mid-to high-intensity aerobic exercise, and to ensure that 10 million people have minimal physical activity.
The initiative presents strategies for improving physical activity as follows: establishing an activity-friendly route to everyday destinations, promoting access to places for physical activity, creating programs for school and youth, implementing community-side campaigns, providing social support and individual support, and providing prompts to encourage physical activity on the basis of equitable and inclusive policy and support. The implementation of each policy is monitored in accordance with the relevant guidelines.
3. Japan: Health Japan 21 (the Second Term)
The Japanese institutions that play a primary role in policies related to the promotion of physical activity are the Ministry of Health, Labor, and Welfare and the Ministry of Education, Culture, Sports, Science, and Technology. The goal of the Ministry of Health, Labor, and Welfare is to prevent non-infectious diseases by promoting physical activity, while the goal of the Ministry of Education, Culture, Sports, and Science is to conduct physical education classes and recreational sports programs. Under this goal, Healthy Japan 21 was introduced as a national health promotion policy in 2000.
Health Japan 21 (2nd term) is Japan’s 21st century health policy that focuses on living free of disease and improving quality of life instead of simply extending life. The focus has shifted from improving health indicators for the entire population to achieving the ideal health status of each individual. It aims to extend life expectancy and reduce health disparities, set indicators for setting goals for the social environment, and presents its own indicators and recommendations related to improving daily life habits and the social environment [34].
The key action goal of Health Japan 21 was to increase the average number of steps per person per day by approximately 1,500 steps from 2013 to 2022. Specifically, the goal for adults aged 20 to 64 was 9,000 steps from 7,841 steps for men and 8,500 steps from 6,883 steps for women. The goal for adults aged 65 years or older was 7,000 steps from 5,628 steps for men and 6,000 steps from 4,584 steps for women. Another goal was to increase the number of adults with regular exercise habits by approximately 10% within 10 years. Japan defines the term ‘exercise habit’ as at least 30 minutes twice a week for 1 year. This is different from the global physical activity guidelines. The goal was to increase the satisfaction rate of exercise habits for men aged 20 to 64 from 26.3% to 36.0% and for women from 22.9% to 33.0% from 2010 to 2022. Men aged 65 or older increased from 47.6% to 58.0% and women from 37.6% to 48.0% from 2010 to 2022.
4. China: Healthy China 2030 Action Plan
In 2016, China established and implemented a government plan called “Healthy China 2030” as part of an effort to build a healthier country. To achieve detailed plans related to this, a new 5-year National Fitness Program (NFP) was announced on August 3, 2021, to improve the physical strength and health of the entire nation [35]. The goal of the plan was to increase the practice rate of physical activity from 37.2% to 38.5%. In this regard, it declared ways to strengthen infrastructure, such as expanding the supply of national-level sports stadiums and facilities, promoting fitness activities for key population groups, such as youth and the elderly, and strengthening the overall development of the sports industry. Specifically, by 2035, the government will increase the supply of fitness facilities within a 15-minute walk to the community and allocate an average of 2.16 sports instructors per 1,000 people to improve the environmental conditions for public access to physical activities. It also suggests accelerating digital innovation in the sports industry and NFP as a roadmap. To solve health problems such as obesity among teenagers, the government will select youth health promotion projects as one of its focus projects to improve sports facilities and equipment standards to allow teenagers to secure 1 hour for sports every day.
STRATEGIES TO PROMOTE PHYSICAL ACTIVITY
Promoting physical activity will not only increase the health and quality of life of people, but also lower medical expenses and develop communities. To raise the level of physical activity, the government, social organizations, and academia should make efforts altogether, and the preparation of the plan must be based on evidence [36]. We will describe the intervention strategy to promote physical activity in terms of primary medical care and national policy.
1. Primary Care-Based Strategies
Mixed results exist as to whether the healthcare system can effectively improve physical activity; however, it was observed that primary care or face-to-face interventions provided by the community play a role in increasing physical activity for 12–24 months [37]. Strengthening counseling on physical activity has been known as a cost-effective method of intervention [38]. Establishing and strengthening a patient evaluation and counseling system to promote physical activity is one of the main axes in the global action plan on physical activity 2018–2030 by WHO [1]. In addition, the UK National Institute for Health and Care Excellence recommends that primary care physicians provide patients with simple physical activity advice and observations during follow-up [39].
There are many theories and methods for physical activity counseling, including the five As (Assess, Advise, Agree, Assist, and Arrange), which is a step-by-step evidence-based approach used worldwide in various healthcare settings [40]. It assesses the level of physical activity, advises on the increase in activity, agrees on individualized plans, and provides continuous strategies to help achieve goals and establish future plans. Traditional exercise prescriptions provided by the American College of Sports Medicine include four components: frequency, intensity, time, and type [41]. Patients should be educated on specific protocols and methods to increase the physical activities and promoted for health care professionals, including clinicians. Additionally, since time constraints have been restricted to physical activity counseling, it is necessary to establish economic and institutional incentives and systems so that appropriate counseling can be conducted in the primary medical environment [40].
2. National Strategies
An increasing number of countries, including the WHO, have established comprehensive plans to promote physical activities at the national level. Under the leadership of the Ministry of Health and Welfare and the Institute for Health Promotion in Korea, the National Health Promotion Plan was adopted 5 times from 2002 to 2021, and each plan has been gradually improved to reflect the global trend of physical activity paradigm shift [42]. The latest Fifth National Health Promotion Plan (HP2030) aims to improve the practice rate of adult aerobic exercise to 53% by 2030, from 47.6% in 2018, and the details are as follows: (1) establishment of physical activity programs and infrastructures on a community basis; (2) development and provision of individualized services to encourage physical activity; and (3) creating a physical activity-friendly environment and strengthening accessibility [43].
In the process of implementing the above program, an individual approach that considers age, sex, residence, and socioeconomic level is required. In particular, a separate plan for groups with poor access to physical activity is necessary to consider equity so that individuals of all ages and abilities can improve their physical activity. A system for monitoring policies and evaluating their effectiveness is important. Moreover, long-term partnership of related departments to promote physical activity is crucial [42].
PANDEMIC AND PHYSICAL ACTIVITY
With the emergence and spread of coronavirus disease 2019 (COVID-19), caused by a novel coronavirus, severe acute respiratory syndrome coronavirus-2 virus, the WHO declared a worldwide pandemic on March 11, 2020.44) Since then, more than 100 countries have implemented quarantine measures and social distancing to protect their citizens from infection and death. Accordingly, participation in physical activities was discouraged due to restrictions on the use of exercise facilities, telecommuting, and online classes [45]. In a study involving participants from 15 countries with restrictions, moderate- and high-intensity exercise decreased by 41% and 42.2%, respectively, after restrictions, and the prevalence of regular aerobic physical activity decreased from 80.9% to 62.5% [46]. In a review of the impact of the pandemic on physical activity, Stockwell et al. [47] analyzed 66 cross-sectional studies and cohort studies, including adults, children, and adolescents, and reported decreases in physical activity and increases in sedentary life from 64 studies. According to some studies, the degree of decrease tended to be higher in groups that were more active before the pandemic [47]. A recent meta-analysis published in February 2022 analyzed changes in physical activity after the pandemic in 14 countries, including Italy, the United States, China, Japan, Spain, Singapore, and Korea, and revealed a decrease in physical activity measured by indicators such as daily steps, moderate and high-intensity physical activity time, and metabolic equivalent task-minutes per week [48].
In Korea, a study based on the Korean Community Health Survey conducted in 2019 and 2020 revealed a decrease in the time spent on moderate-intensity physical activity, which was more than 20 minutes per week for both men and women [49]. In a study of 834 adults in Korea, the number of daily steps measured by smartphone applications before and after the COVID-19 pandemic decreased by more than 10% from approximately 6,747 to 5,812 [50]. A study involving 1,154 adults in Korea reported that the average daily sitting time increased by 44 minutes after the pandemic [51]. Among children and adolescents in Korea, a decrease in physical activity and weight gain due to the pandemic was also observed [52]. An increase in obesity and chronic disease prevalence due to a decrease in physical activity and changes in other lifestyle habits was also observed. According to a study by the Korean Society for the Study of Obesity, 46% of adult participants showed weight gain after the pandemic [53]. Additionally, Korea Centers for Disease Control and Prevention reported that the prevalence of hypertension and hyperlipidemia in men increased significantly when comparing the results of the 2019 and 2020 KNHANES [54].
It has been reported that physical activity is associated with chronic diseases and has a positive immunological effect, which can act as a protective factor against the incidence and severity of infection. According to a study involving adults in Korea, regular physical activity significantly lowered the incidence, severity, and mortality of COVID-19 [55]. In addition, depression and stress increased due to self-isolation and social distancing during the pandemic [56], and this phenomenon further emphasizes the importance of physical activity, considering its benefits to mental health. Accordingly, several documents have presented guidelines for practicing physical activity during the restriction period. Representatively, there are home-based exercises, exercises using electronic-based platforms such as YouTube or applications on smartphones and/or tablets, and participation in online exercise classes [57,58]. Non-contact physical activities such as walking, jogging, and cycling are also emphasized, rather than physical activities in enclosed spaces. As an alternative to group exercise and participation in group classes, exercise with a spouse or family (such as jump rope, badminton, and table tennis) is recommended [59]. It is important to note that physical activity in infectious diseases and other contraindications is not recommended, and excessive exercise such as high-volume high-intensity training may lower immunity and increase susceptibility to infection; hence, the intensity of exercise should be determined individually [60].
CONCLUSION
The major guidelines recommend that adults perform 150–300 minutes of moderate-intensity physical activity, 75–150 minutes of vigorous-intensity physical activity, or an equivalent combination of these activities, and more than twice of the muscle strengthening activity per week. In addition, they suggested reducing sedentary behavior in all age groups. However, physical activity has not significantly improved globally since 2001, and the prevalence of physical inactivity has been 1 in 4 as of 2016. In Korea, aerobic physical activity continues to decrease, and more than half of adults and more than 90% of adolescents are not active enough. Only 16.9% of adults practiced both the aerobic and muscle-strengthening activities sufficiently, and the prevalence was lower in women, elderly, and those in the rural areas. Sedentary time has been consistently increasing, at approximately 8.6 hours a day in adults and more than 10 hours in adolescents.
The WHO has developed a global action plan to help each country develop policies to promote physical activity. In addition, many countries, including the United States, Japan, and China, have created guidelines, introduced policies, and improved infrastructure to promote physical activity. To increase the level of physical activity, the government, academic institutions, social organizations, schools, workplaces, and individuals should recognize the seriousness of the current situation and make efforts to fix it. Interventions should include clinical and policy approaches. Appropriate education, promotion, and systems are necessary so that health professionals can provide counseling and advice on physical activity to patients. Policy approaches include promoting and educating people on physical activities and creating a physical activity-friendly environment. When introducing and implementing policies, it is crucial to consider equity and individual characteristics. In addition, the effectiveness of the policy requires monitoring, and partnership of multiple sectors is important. Physical activity levels have significantly reduced during the COVID-19 pandemic, posing a threat to the physical and mental health of people. There are numerous recommendations to promote practicable exercise in social distancing, which should be further embodied and improved through research in the future.