INTRODUCTION
Childbearing is one of the primary topics in demographic science and a social issue in every society. Fertility is known to be the most important phenomenon determining population fluctuations, and studying the phenomenon is important. Hence, demographic policies in most countries focus on either reducing or increasing fertility [1]. One of the most significant demographic changes over the last three decades has been a sharp decline in the total fertility rate (TFR) worldwide, especially in developing countries [2]. Iran is a developing country that has experienced a sharp decline in fertility [3]. This declining trend has been so significant that the TFR has decreased from 6.3 in 1986 [4] to 1.98 in 2000, and in 2018, it reached 1.62 [5].
Declining fertility below the replacement level has significant negative effects on economic, social, and cultural structures. One of adverse consequences of low fertility is a change in population structure, called population aging, which results in a lack of economic growth and development, a lack of social welfare, and the imposition of heavy costs on the health system [6]. Therefore, population policies that reduce these impacts have been considered [7]. However, any population policy and planning measure must consider all contributory aspects. Therefore, it is necessary to attain a correct understanding of the formation of childbearing behavior, as well as the intention to have children, as intention is a key factor and immediate determinant of childbearing behavior [1].
This issue is often examined within the framework of the theory of planned behavior (TPB) in demographic research [8]. The applicability of the TPB in fertility has been demonstrated in several studies [1,8-10]. However, several other factors affect the childbearing behavior, including individual, family, social, economic and cultural factors [2]. After a study has determined the factor that affects fertility behavior, the TPB allows us to examine this finding by tracking the effects of the said factor on three immediate determinants of childbearing intention [9]. One of the factors affecting childbearing, especially in Iranian society and that has been proven by several studies, is social support [11,12]. Therefore, the present study added this concept to the TPB and developed it. Consequently, an extended theory of planned behavior (ETPB) was used as a conceptual framework for this study.
Based on the available evidence, most previous studies on childbearing have used questionnaires that were not designed based on the results of qualitative studies, but were based solely on TPB constructs [9]. Due to the lack of a valid questionnaire based on ETPB constructs, this study was conducted to determine the validity and reliability of a questionnaire designed to examine factors related to childbearing intentions and behaviors in Iranian society.
METHODS
This mixed-methods study was conducted in Hamadan city, western Iran, in 2021. This study was approved by the Ethics Committee of the University of Medical Sciences, under the code of ethics IR.UMSHA. REC.1397.847. Informed consent was obtained from all study participants. This study was conducted in two phases: generating items and measuring the psychometrics of the scale.
1. The Item Generation
Item generation is usually performed through comparative and/or inferential methods [13]. Both methods were used to generate the items in the present study. The comparative method requires an extensive review of the literature to achieve theoretical conception of the construct under study; therefore, an extensive literature review related to the TPB and factors related to childbearing was also conducted. To achieve the specific conception of factors related to childbearing, a qualitative study was conducted using a directed content analysis approach through interviews with 17 people [14]. The participants were married women and men.
The independent variables were nine factors, organized into a logical framework, including (1) behavioral beliefs, (2) evaluation of behavioral outcomes, (3) normative beliefs, (4) motivation to comply, (5) control beliefs, (6) perceived power, (7) informational support, (8) instrumental support, and (9) emotional support. In total, 116 items were extracted from these variables, following which a 5-point Likert scale was used to score them. The number of items extracted for each sub-construct of the ETPB and how they were scored is as follows: both behavioral beliefs and outcome evaluations of childbearing were assessed using 20 items each. For behavioral beliefs, the items were rated on a 5-point scale, ranging from 1 (strongly agree) to 5 (strongly disagree). In the outcome evaluation, the items were rated on a 5-point scale, ranging from 1 (very high) to 5 (very low). Higher scores indicate a more positive attitude toward childbearing.
Normative beliefs and motivation to comply with childbearing were assessed using 10 items each. For normative beliefs, the items were rated on a 5-point scale, ranging from 1 (strongly agree) to 5 (strongly disagree).
For motivation to comply, the items were rated on a 5-point scale, ranging from 1 (very high) to 5 (very low). Higher scores indicate more subjective norms persuasive toward childbearing.
Both control beliefs and perceived power were assessed by 18 items each and were rated on a 5-point Likert scale, ranging from 1 (very high) to 5 (very low). A higher score indicated greater perceived control over having a child.
Informational, instrumental, and emotional support in childbearing were assessed using seven, six, and seven items, respectively. These items were rated on a 5-point scale, ranging from 1 (always) to 5 (never). Higher scores indicated greater social support in childbearing. All items for informational, instrumental, and emotional support were scored in reverse order. It is worth noting that the questionnaire was compiled in the Persian language.
2. Psychometric Properties
This phase consisted of examining the content, face, and construct validity of the Iranian version of the theory-based childbearing beliefs questionnaire. Furthermore, the reliability of the scale in terms of its internal consistency and stability was examined.
1) Content validity
Content validity was assessed both qualitatively and quantitatively by 12 health education, promotion, and demographic specialists. In the qualitative method, specialists reviewed the questionnaire to check its grammar, wording, item allocation, and scale. Quantitative content validity was assessed by calculating the content validity ratio (CVR) and content validity index (CVI). To calculate the CVR, specialists were asked to assess each item on a 3-point Likert scale (1=essential, 2=useful but not essential, 3=not essential). To calculate the CVI, 12 expert panelists were asked to determine the relevance, clarity, and simplicity of each item using a 4-point Likert scale. Based on Lawshe’s table, the items with CVR <0.56 and CVI <0.79 were removed [15].
2) Face validity
Facial validity was applied in two phases: qualitative and quantitative. In the qualitative method, five individuals similar to the target group were interviewed face-to-face, to examine the relevance, complexity, and ambiguity of the items. To remove irrelevant items and determine the importance of each item, the item impact score was used as a quantitative method. In this regard, a 5-point Likert scale was used for each item (5=completely important, 4=important to some extent, 3=moderately important, 2=slightly important, 1=not important at all). The questionnaire was administered to 10 people who were similar to the target group.
To calculate an item impact score, we first calculated the percentage of individuals who scored 4 or 5 on item importance (frequency) and the mean importance score of the item (importance). The item impact score of instrument items was then calculated using the following formula: item impact score=frequency×importance. If the item impact of an item was equal to or greater than 1.5, corresponding to a mean frequency of 50% and an importance mean of 3 on a 5-point Likert scale, it was maintained in the instrument; otherwise, it was eliminated.
3) Construct validity
Exploratory factor analysis (EFA) was performed to assess the construct validity of the instrument to extract latent factors and determine the dimensionality of the scale. EFA was performed using the principal component analysis (PCA) extraction method, utilizing varimax rotation Kaiser normalization. Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity were used to assess the adequacy of the sample size for the factor analysis. KMO values of 0.7–0.8 were considered good and 0.8–0.9 were considered large [16]. Eigenvalues greater than 1 were used to determine the number of factors. Factor loadings equal to or greater than 0.4 were considered appropriate [17].
Although different recommendations were given regarding the sample size for factor analysis, a common recommendation is to select five or 10 participants per item [18]. In this study, five participants were considered per item. Therefore, considering that the examined instrument entered the stage of assessment of construct validity with 64 items, the sample size included 320 participants.
Inclusion criteria for participants were married women aged less than 35 years and married men whose spouses were under 35 years of age who lived in Hamadan city, western Iran, in 2021. This group was chosen because the intention to have children is more greatly affected by the current situation and the near future of the living conditions and society of prospective parents. Therefore, the fertility level of society in the future depends significantly on the fertility intention of the mentioned group [1]. In this study, sampling was performed using a stratified cluster sampling method. The population covered by each of the comprehensive health service centers in the city of Hamadan was considered a cluster. In total, 20 health centers were included in the study. Estimation of the sample size for each cluster was performed by probability proportional to the size of the population in each of the 20 health centers. In each cluster, the gender variable was considered as a stratification criterion, so that sampling could be performed in equal proportions in both genders. The first household in each cluster was randomly selected, and sampling was continued until the desired number of samples in each cluster was reached. In the selected household, a man or woman eligible to participate in the study was asked to participate.
In addition, confirmatory factor analysis (CFA) was conducted to assess how well the model extracted by the EFA and the theoretical framework behind the instrument fitted the observed data. The standard goodness-of-fit indices used in CFA were χ2/degrees of freedom (df) <3, comparative fit index >0.9, normed fit index >0.9, goodness of fit index >0.9, Tucker-Lewis index >0.9, and root mean square error of approximation <0.08 [19]. In addition, convergent validity and discriminant validity were examined. When the correlation between items was high, they belonged to a specific construct with acceptable convergent validity. The condition for acceptable convergent validity is an average variance extracted (AVE) >0.5, composite reliability (CR) >0.7, and CR>AVE. Discriminant validity means that the items of one construct are not highly correlated with the items of another construct and differ from each other. Discriminant validity was obtained by calculating the maximum shared squared variance (MSV) and average shared squared variance (ASV), and the values of MSV and ASV should be less than AVE [20].
Data were analyzed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA) and AMOS Graphics ver. 24.0 (IBM Corp.).
4) Reliability
Internal consistency and stability were used to determine the instrument reliability. To measure internal consistency, the Cronbach’s alpha (α) coefficient was calculated for each construct separately and for all constructs as a whole. The α-values of 0.7 to 0.8 were regarded satisfactory [21]. Furthermore, to assess the stability, test-retest reliability was performed using the intraclass correlation coefficient (ICC) for 30 participants with a 2-week interval. Based on the 95% confidence interval of the ICC estimate, values less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9, and greater than 0.90 are indicative of poor, moderate, good, and excellent reliability, respectively [22].
RESULTS
The total number of participants was 320, with a mean age of 29.94±7 years and a mean marriage duration of 7.56 years. Table 1 presents the demographic characteristics of the participants. Instrument validation for different aspects is as follows:
1. Content Validity
Based on the qualitative content validity, 10 items were removed. To calculate the CVR, based on Lawshe’s table, items that scored greater than or equal to 0.56 were kept on the scale. During this phase, 28 items were removed. To calculate the CVI, in accordance with Waltz and Baussel [23], items with CVI values greater than or equal to 0.79 were accepted, and 14 items that did not meet this criterion were deleted. In total, 64 items were entered into the next step after performance of qualitative and quantitative content analyses.
2. Face Validity
At this stage, none of the items were removed, but two items were modified based on the participants’ suggestions. The results of the quantitative face validity showed that the impact score of all items was greater than 1.5.
3. Construct Validity
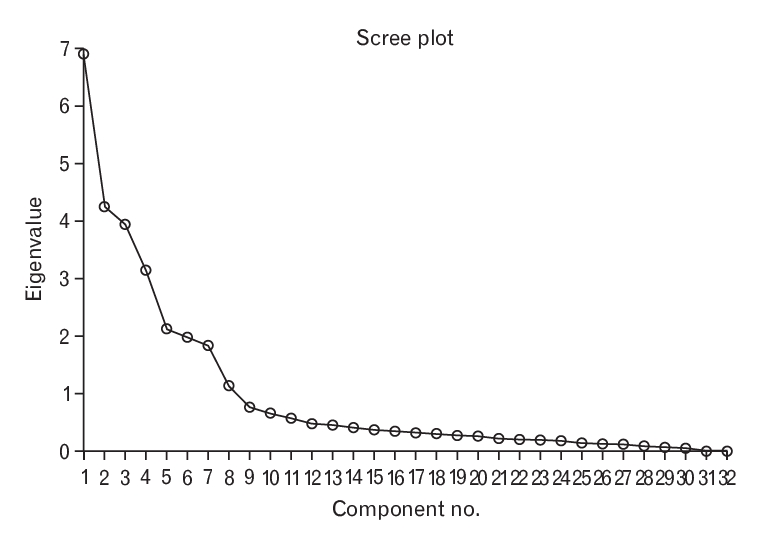
The value of KMO=0.703 demonstrated that the data were appropriate for factor analysis, and Bartlett’s test results with χ2 (df=496) 9,456.61 (P<0.001) showed that factor analysis based on the correlation matrix was acceptable and that discoverable relationships existed between the variables. Latent factors were extracted using a PCA and varimax rotation. In this model, eight factors were extracted, according to eigenvalues greater than 1 and the scree plot in Figure 1.
The eight latent factors had eigenvalues of 6.9, 4.24, 3.94, 3.14, 2.12, 1.98, 1.84, and 1.13. In total, the eight extracted factors explained 79.1% of the total variance of the instrumental variables. The factor loadings of all the items were equal to or greater than 0.4. The results of EFA are presented in Table 2.
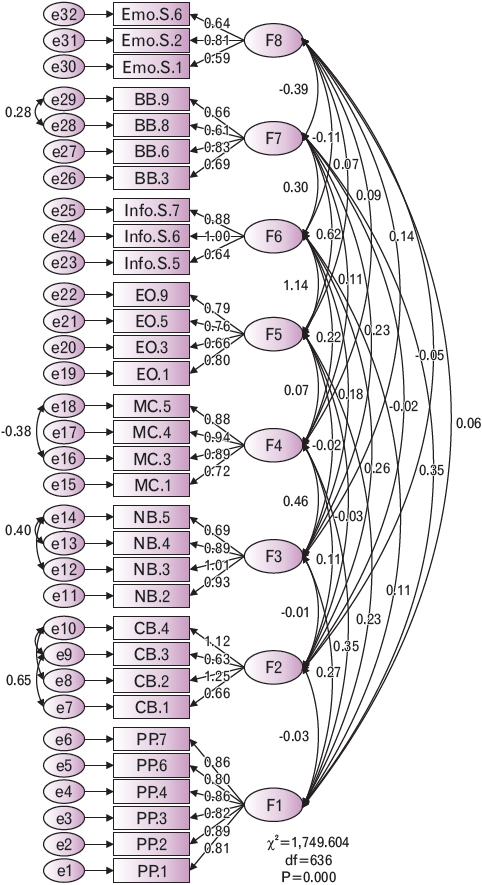
The factors identified in the model were: (1) factor 1 (perceived power), with six items; (2) factor 2 (control beliefs), with four items; (3) factor 3 (normative beliefs), with four items; (4) factor 4 (motivation to comply), with four items; (5) factor 5 (evaluation of behavioral outcomes), with four items; (6) factor 6 (informational support), with three items; (7) factor 7 (behavioral beliefs), with four items; and (8) factor 8 (emotional support), with three items. A total of 32 items were obtained from the EFA. Based on the results of the EFA, one of the factors of the logical framework—namely, instrumental support—was removed because all of its items demonstrated cross-loading with other factors.
The results of the CFA of the general model with 32 items in eight subscales showed that the model was acceptable in its current form (Figure 2).
The CFA indices are presented in Table 3. Therefore, CFA shows the adequacy of the model and the proper fit of its structural model for the study population. The results of the convergent and discriminant validity assessments are presented in Table 4. The results indicate that the ETPB constructs had good convergent and discriminant validity.
4. Reliability
Reliability was evaluated using internal consistency. Cronbach’s α coefficient for the subscales ranged from 0.71 to 0.93. In addition, the ICC for the questionnaire subscales was calculated and ranged from 0.74 to 0.94. Cronbach’s α and ICC of the theory-based childbearing questionnaire subscales are shown in Table 4.
DISCUSSION
This study aimed to develop and validate an instrument for assessing married men and women’s intentions to bear children. The TPB provides an appropriate theoretical framework that can be used to explain human social behavior [24]. One of these behaviors is childbearing, which is influenced by many factors [2]. In Iranian society, one of the factors affecting childbearing is social support [11,12]. Therefore, the concept of social support was added to the TPB and an extended model of the TPB (i.e., ETPB) was used as a theoretical framework in this study. The questionnaire designed in the present study is a valid and reliable scale for examining and measuring factors related to childbearing intentions and behaviors, based on the ETPB, in the Iranian social and cultural context. Comparative and inferential approaches were used simultaneously to achieve a relatively comprehensive and complete perception of theoretical concepts. Along with observing the principles of designing and extracting items, demographics and cultural conditions were also considered.
In this mixed-method study, to generate items, an extensive literature review and qualitative study with a directed content analysis approach were performed. In the studies conducted by Babak et al. [25] and Darabi et al. [26], in addition to literature reviews, qualitative study findings were used to generate items. The use of qualitative studies to generate items makes it possible to obtain more accurate and comprehensive information from individuals’ views and beliefs. The generated items would help researchers to correctly and precisely measure the concepts examined in this study.
In the present study, the content validity of the instrument, with the aim of determining whether the items fully evaluated the construct or not [27], with the help of experts who were familiar with the ETPB constructs and calculated the CVI and CVR, was performed. The mean scores for the CVR and CVI were 0.95 and 0.96, respectively. The values obtained in this study were reasonable and satisfactory. In our study, the opinions of 12 experts with experience in instrument-making in the field of childbearing research were used to calculate the CVR and CVI. For face validity, none of the items were removed, and only two items were modified in accordance with the participants’ suggestions. Thus, it can be concluded that the questionnaire items were sufficiently relevant, simple, and understandable.
The most important step in assessing the validity of the questionnaire is to determine its construct validity, especially in the process of psychometrics. Factor analysis is the best method in this field [28]. Based on the results of the present study, the value of the KMO index for all structures was 0.703, which indicates the adequacy of the sample size and favorable factor analysis [29]. In this study, the null hypothesis of data sphericity was rejected, and the KMO statistic was confirmed.
The EFA in this study was conducted for ETBP constructs, and the number of extracted factors based on the items used in the questionnaire was determined by the scree plot and eigenvalues. In total, 32 items were removed from the original questionnaire. Eight factors were extracted that explained 79.1% of the variation in the constructs developed in the questionnaire. This result indicated the strong predictive power of these factors. In the present study, the results of CFA showed that the data had a sufficient fit with the eight proposed constructs and reached an acceptable threshold [30].
The reliability of the questionnaire was assessed using internal consistency (Cronbach’s α) and test-retest tests. The internal consistency results showed that the developed questionnaire had an acceptable reliability. The study revealed an internal consistency of 0.71–0.93 for subscales. Additionally, an internal consistency of 0.85 was reported for the ETPB. However, there was no significant increase in Cronbach’s α coefficient when any items were deleted. These findings are consistent with the results of a study conducted by Erfani [1], who used the TPB. In addition, ICC demonstrated appropriate stability for the scale, as it was examined by 30 participants with a 2-week interval, ranging from 0.74–0.94 and 0.84 ETPB. This result indicates that the developed questionnaire has significant stability and can provide reliable results at different times and places.
The unique aspects of our tool include its ability to assess numerous psychological factors related to childbearing intentions and behaviors through indirect measurements of TPB constructs, which may help to better identify specific targets for behavioral change and improve evaluation of psychometric properties. Moreover, the new construct, “social support,” in its role as an important determinant of childbearing intentions and behaviors, was added to the TPB. Additionally, a suitable qualitative study was conducted to develop an item pool for the questionnaire.
In general, considering the acceptable validity and reliability of the proposed instrument, the developed questionnaire would be a suitable self-report scale to examine and study factors related to childbearing intentions and behaviors. This instrument requires further testing among other populations in Iran.
The developed questionnaire is a valid and reliable tool for evaluating belief-based determinants of childbearing intentions and behaviors among married men and women in Iran. The final version of this tool is provided in the Supplement 1.