INTRODUCTION
The practice of skipping regular meals, whether for dietary purposes or simply due to the demands of a busy daily life, has become prevalent. In South Korea, the rate of skipping breakfast has steadily increased from 21.4% in 2011 to 34.6% in 2020, as reported by national health statistics [1]. These lifestyle changes have contributed to a significant increase in cardiometabolic risk factors (CMRF), including obesity, dyslipidemia, and type 2 diabetes [2,3]. The prevalence of metabolic syndrome is on the rise in South Korea. This poses a significant concern, as metabolic syndrome-associated risk factors are linked to a higher likelihood of developing chronic diseases [4].
The association between irregular eating patterns, such as skipping meals or reduced meal consumption frequency, and various health conditions or illnesses has been actively explored. Research indicates that skipping breakfast is associated with elevated cholesterol and blood pressure levels, as well as increased rates of obesity, metabolic syndrome, and cardiovascular disease [5,6]. Moreover, skipping breakfast has been linked to higher average blood glucose levels over a 24-hour period [7], impacting postprandial blood glucose elevation and insulin sensitivity, resulting in an increased risk of diabetes [8]. A recent study with a national population-based sample of young Australian adults revealed that higher eating frequency was associated with decreased cardiometabolic risk factors and improved lipid profiles [9]. In a study involving South Korean adults, people who consumed two or less than two meals per day had significantly higher odds of metabolic syndrome than those who ate three regular meals [10]. Therefore, a higher frequency of regular meal consumption is beneficial in patients with metabolic syndrome.
Although numerous studies have investigated the relationship between breakfast consumption, meal frequency, and metabolic syndrome in Korea, more specific research on its association with all types of regular meal skipping including lunch and dinner is limited and inconsistent. While some studies have reported fewer abnormalities in individuals who skip dinner compared to those who skip breakfast [11,12], other studies have observed that skipping dinner is linked to increased obesity rather than skipping breakfast [13].
In this study, we aimed to explore the correlation between skipping breakfast, lunch, and dinner and the risk factors for cardiovascular and metabolic diseases among Korean adults. Although many studies have reported the association of skipping meals or the frequency of meals with metabolic syndrome, no prior research has yet analyzed how or whether different types of meal skipping have different effects on cardiometabolic risk factors. Therefore, investigating the differences in the significant effects of various meal skipping patterns could provide a sound basis for dietary behavioral recommendations that promote cardiometabolic health.
METHODS
1. Data Collection and Study Population
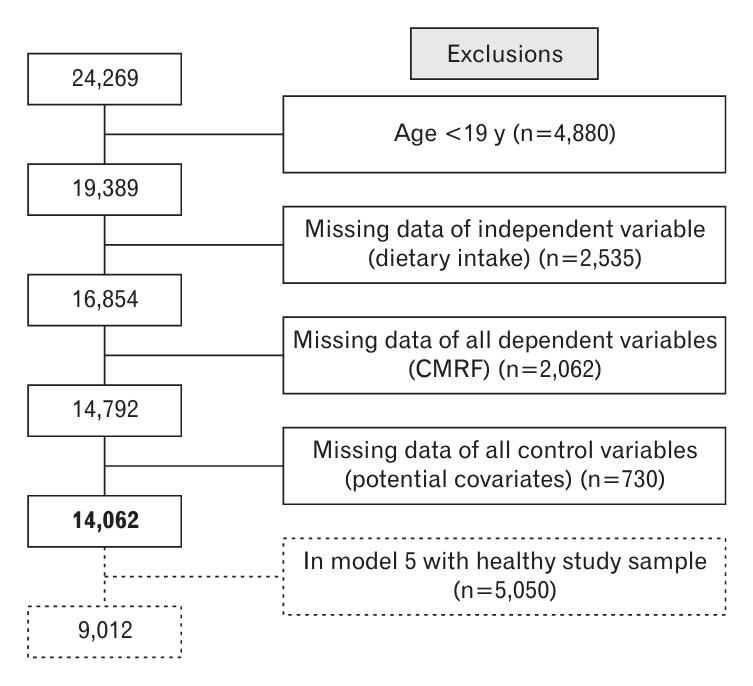
This cross-sectional study examined the association between cardiometabolic risk factors and specific meal skipping habits in Korean adults. We used data from the 7th Korea National Health and Nutrition Examination Survey (KNHANES) (2016ŌĆō2018) which is a nationwide survey conducted by the Korea Disease Control and Prevention Agency (formerly, Korea Centers for Disease Control and Prevention) consisting of health, behavioral, and dietary surveys, standardized physical examinations, and laboratory tests. Among the 24,269 participants registered in the 7th KHANES (2016ŌĆō2018), participants under the age of 19 years (n=4,800), with missing data on dietary intake (n=2,535), anthropometric and biochemical measurements of cardiometabolic risk factors (n=2,062), and sociodemographic and lifestyle variables that were potential confounding variables (n=730) were excluded. Thus, ultimately a total of 14,062 individuals were included in the study population (Figure 1). The study was approved by the Institutional Review Board (IRB) of the Samsung Medical Center (IRB no., SMC 2023-03-127). Informed consent was obtained from all individual participants included in the study.
2. Diet Survey and Categories of Regular Meal Skipping
We categorized the types of irregular meal consumption into eight categories (hereinafter ŌĆ£groupŌĆØ) using the dietary survey undergone in the 7th KNHANES. Participants were asked to report the usual frequency of weekly breakfast/lunch/dinner consumption in the previous year. Initial responses for meal consumption frequency (5ŌĆō7 times a week, 3ŌĆō4 times a week, 1ŌĆō2 times a week, 0 times a week), were categorized into a binary variable ŌĆ£regularŌĆØ (5ŌĆō7 times a week) and ŌĆ£irregularŌĆØ (0ŌĆō4 times a week) breakfast/lunch/dinner consumption. Thus, eight different dietary habits were defined (Table 1): First, the regular consumption of all three meals was defined as group 1 (regular eater group, RE group). Regular consumption of breakfast and lunch but skipping dinner was defined as group 2 (irregular dinners group, ID group). Regular consumption of breakfast and dinner but skipping lunch was defined as group 3 (irregular lunches group, IL group). Group 4 (irregular breakfast group, IB group) was defined as the regular consumption of lunch and dinner but skipping breakfast. Regular skipping of lunch and dinner, but consuming regular breakfast, was defined as group 5 (irregular lunches and dinners group, ILD group). Patients who regularly skipped breakfast and dinner but consumed regular lunch were defined as group 6 (irregular breakfast and dinner group, IBD group). Group 7 (irregular breakfast and lunch group, IBL group) consisted of regular skipping of breakfast and lunch but regular consumption of dinner. Finally, group 8 (irregular eater group, IBLD group) was defined as having a meal skipping habit for all three meals. In this study, irregular meal consumption and meal skipping were used as interchangeable definitions.
3. Anthropometric and Biochemical Measurements: Cardio-metabolic Risk Factors
Anthropometric variables, such as height, weight, blood pressure, and biochemical variables, were measured using standardized procedures. Systolic and diastolic blood pressures (SBP and DBP, respectively) were measured three times, and the average values of the second and third measurements were used. The survey data included total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride, and fasting blood sugar (FBS) levels, which were measured after fasting for at least 8 hours. Hemoglobin A1c (HbA1c) and high-sensitivity C-reactive protein levels were measured using standard procedures.
4. Covariates
We included potential confounding factors, such as sociodemographic characteristics (age, sex, household income, education level, and work shift), lifestyle factors (smoking status, alcohol consumption, physical activity, and energy intake), body mass index (BMI), and history of chronic diseases (hypertension, hyperlipidemia, diabetes, stroke, and coronary heart disease). BMI was calculated by dividing body weight by height squared (kg/m2). Household income levels were categorized as low, middle-low, middle-high, and high based on monthly household income quartiles. Educational level was classified as below elementary school, middle school, high school, and college or higher. Work shift was divided into day shift, swing, night shift, and unemployed. We defined ŌĆ£physically activeŌĆØ as at least 150-minute moderate intensity activity, or at least 75-minute vigorous intensity activity, or an equivalent combination of moderate and vigorous intensity activities per week. Participants who smoked more than 100 cigarettes in their lifetime and were still smoking were defined as ŌĆ£current smokers.ŌĆØ Participants who had never drunk any alcoholic beverages or less than once a month during the past year were categorized as ŌĆ£noŌĆØ alcohol consumption. Daily energy intake was calculated based on the 24-hour dietary recall data. All data were collected by trained staff using standardized protocols. A history of chronic diseases was collected using a self-reported physicianŌĆÖs diagnosis.
5. Statistical Analysis
We performed an analysis of variance (ANOVA) for continuous variables and the Pearson chi-square test for categorical variables to compare general characteristics and ANOVA for cardiometabolic parameters according to the above-specified meal consumption habits. We reported the percentages and mean┬▒standard deviations for categorical and continuous variables, respectively.
We conducted multiple linear regression (MLR) analyses to investigate the association between meal skipping and cardiometabolic risk factors. In the first MLR model, we adjusted for age, sex, household income, educational level, work shift, regular physical activity, smoking status, alcohol consumption, hypertension, hyperlipidemia, diabetes, stroke, myocardial infarction, angina, total energy intake, and BMI (model 1). We additionally adjusted for the intake of hyperlipidemia medication (model 2), hypertension medication (model 3), or diabetes medication (model 4) according to the related dependent variables (total cholesterol, HDL-C, LDL-C, calculated LDL-C, triglyceride, SBP, DBP, HbA1c, and FBS).
In addition, we analyzed the estimated effects of individual types of meal skipping on cardiometabolic risk factors through their predicted values and mean differences based on group 1 (RE group) to present the differences numerically.
Furthermore, we conducted a subgroup analysis excluding all participants diagnosed with any chronic diseases (hypertension, hyperlipidemia, diabetes, stroke, myocardial infarction, and angina), as a robustness check with so-called ŌĆ£healthy participantsŌĆØ only (model 5). Among participants diagnosed with any of the above diseases at least 73% or as much as 80% were ŌĆ£REs.ŌĆØ One could possibly assume that such habits came with their diagnosed diseases due to external binding factors, such as the intake of drugs or prevention of health deterioration. Thus, we cannot rule out the possibility of a biased population since participants diagnosed with any kind of chronic disease might have adopted regular eating habits as an approach to health management. For such reason we have created and investigated the ŌĆ£healthy onlyŌĆØ study population (N=9,012) in our subgroup analysis to confirm the robustness of our results.
Statistical significance was set at P<0.05. All statistical analyses were performed using the Stata ver. 15.0 software (STATA Corp., College Station, TX, USA).
RESULTS
1. Basic Characteristics according to Main Meal Consumption Habits
The majority of participants in the 7th KNHANES (2016ŌĆō2018) reported having three regular meals per day (57.74%), followed by irregular breakfast (25.00%), irregular lunch (4.56%), irregular breakfast and dinner (4.03%), irregular breakfast and lunch (3.24%), and irregular dinner (3.07%). The IBD and IBL groups accounted for a proportion similar to that of the IL and ID groups (Table 1). The general characteristics of the participants in the eight groups are presented in Table 2. In general, the female participants had more irregular meal consumption habits. Participants under the age of 50 years, those with middle-high to high household income, those who received high school/college or higher education, or those who drank alcohol tended to have more irregular meal consumption habits, which were more prominent in groups that included irregular breakfast consumption. The number of swing or night-shift workers was higher in the irregular meal consumption group than in the regular meal group. Former smokers had regular meal consumption habits, whereas current smokers had irregular meal consumption habits. The average daily calorie intake was the highest in the IB group (2,072.9┬▒999.9 kcal/d). Notably, participants diagnosed with chronic and cardiovascular diseases such as hypertension, dyslipidemia, diabetes, stroke, MI, and angina generally had more regular meal consumption habits.
2. Cardio-metabolic Parameters according to Main Meal Consumption Habits
Table 3 shows association of cardio-metabolic parameters, including blood pressure, lipid profiles, glycemic profiles, and inflammation marker, by the specified eight categories of meal skipping. In the IB group, total cholesterol, LDL-C, calculated LDL-C, triglycerides, fasting glucose levels and blood pressure readings, were reported significantly higher than in the RE group. In the IL group the lipid profiles, total cholesterol, and calculated LDL-C levels were reported significantly higher than in the RE group. Similarly, in the IBL group the lipid profiles, total cholesterol, and triglyceride levels were reported significantly higher. Moreover, in the IBD group total cholesterol level was significantly higher.
The association between cardiometabolic risk factors and skipping dinner (ID group) was not significant. In contrast, HDL-C levels were reported to be significantly higher in the ID group. Overall, most cardiometabolic risk factors were significantly higher in the breakfast skipping group, followed by the lunch skipping group, and the breakfast and lunch skipping group.
The findings from the main analysis (Table 3) were almost identical in the subgroup analysis that were conducted with the ŌĆ£healthy onlyŌĆØ population (Table 4). The only difference between the results of the two analyses was that the total cholesterol levels were higher in the ILD group than in the RE group. There were no further significant differences in the results, not only in the groups that included irregular breakfast consumption, but also dinner skipping.
3. Predicted Effects on Cardio-metabolic Risk Factors and Mean Differences
We estimated the numerical effects of the individual types of meal skipping on the cardiometabolic risk factors using their predicted values and mean differences. The reference group for mean difference was the regular eater group. As shown in Tables 5 and 6, all predicted mean values of the RE group were mostly within the normal range. Total cholesterol levels increased by 5.16 mg/dL (P<0.001) in the IB group, 4.16 mg/dL (P<0.01) in the IL group, by 6.02 mg/dL (P<0.001) in the IBL group and by 5.03 mg/dL (P<0.001) in the IBD group, all compared to the RE group. LDL-C levels increased by 4.84 mg/dL (P<0.01) only in the IB group compared to the RE group. Calculated LDL-C levels increased by 3.53 mg/dL (P<0.001) in the IB group, 2.84 mg/dL (P<0.05) in the IL group, and 3.74 mg/dL (in healthy only, P<0.05) in the IBL group compared to the RE group. Triglyceride levels increased by 6.78 mg/dL (P<0.01) in the IB group, and 13.18 mg/dL (P<0.05) in the IBL group compared to the RE group. Fasting glucose levels increased by 0.93 mg/dL (P<0.05) in the IB group compared to those in the RE group. Lastly, HDL cholesterol levels increased by 2.1 mg/dL (P<0.001) in the ID group compared to those in the RE group. The results showed that total cholesterol and triglyceride levels were the highest in the IBL group, and that LDL-C or calculated LDL-C levels were higher only in the groups that included dietary habits of breakfast skipping, lunch skipping, or both meals.
DISCUSSION
Our study is the first to investigate whether different meal skipping patterns significantly affect cardiometabolic risk factors in Korean adults. We measured total cholesterol in the IB, IL, IBL, and IBD groups, calculated LDL-C in the IB and IL groups, LDL-C in the IB group, triglyceride in the IB and IBL groups, and FBS in the IB group, which were significantly higher than those in the RE group. Therefore, the findings of our study show that skipping breakfast or lunch, rather than skipping dinner, could increase cardiometabolic risk factors in South Korean adults.
In line with previous research, we reaffirmed that skipping breakfast is associated with increased metabolic risk factors. Earlier studies have shown that breakfast skippers tend to have elevated levels of total cholesterol, LDL-C and triglyceride [14] and are more likely to have metabolic syndrome [6] compared to regular breakfast eaters. A previous study showed that Korean adult breakfast skippers were more likely to have a higher fat intake and were more prone to obesity and metabolic syndrome [15]. Another study reported that skipping breakfast was associated with a higher risk of insulin resistance in people without diabetes and was thus a risk factor for type 2 diabetes mellitus [16]. In another study, breakfast consumption was reported to affect appetite regulation, feelings of satiety, total energy intake, and metabolic efficiency of the diet [17]. Similarly, according to a cross-sectional study using data from the National Health and Nutrition Examination Survey (1999ŌĆō2004) breakfast, which accounts for a larger percentage of daily energy intake, was associated with a lower daily total calorie intake [18].
The knowledge that having regular breakfast can be beneficial in managing and preventing metabolic syndrome is also widespread, possibly because of the difference in nutrient and food group intake between breakfast consumers and skippers. Several studies have indicated that breakfast consumption improves nutrient profile [19]. People who regularly consumed breakfast had a more diverse nutrient intake than breakfast skippers whose intake levels of various nutrients fell below the estimated average requirement. Furthermore, people who skipped breakfast consumed a significantly higher proportion of energy from fat than from carbohydrates in their diet [15,20]. Therefore, skipping breakfast and adopting an imbalanced daily diet could potentially elevate cardiometabolic risk factors. Our results suggest that regular breakfast consumption can potentially contribute to the reduction of cardiometabolic risks, and this effect is likely related to its impact on overall dietary habits.
Furthermore, our results show that reduced meal frequency (less than three regular meals) leads to significantly higher cardiometabolic risk factors, which is also in line with previous findings. Regarding the overall frequency of regular meal consumption, prior studies on European adults showed that a higher eating frequency was associated with decreased cardiometabolic risk factors, especially better lipid profiles [9,21]. Another study on Korean adults claimed that people eating two meals a day had a higher fat intake, were more prone to obesity, and likewise had a significantly higher risk of metabolic syndrome than those who consumed three regular meals [10]. There are several reasons for the correlation between reduced meal frequency and a higher risk of metabolic syndrome; one explanation is that individuals eating only one or two meals per day tend to eat more calories during each meal [22]. Increased insulin secretion owing to a sudden surge in postprandial glucose levels after prolonged fasting can eventually lead to insulin resistance [23]. Reduced meal frequency, higher postprandial hyperglycemia and hyperlipidemia, and higher peaks and subsequently lower troughs of insulin may provoke oxidative stress and contribute to chronic inflammation, leading to the establishment of a mechanistic connection between these factors and the components of metabolic syndrome [11,24].
Another notable finding of our study is that the association between cardiometabolic risk factors and skipping dinner was not statistically significant. Previous findings on the effects of skipping dinner have been inconsistent. Some studies reported that skipping lunch or dinner resulted in fewer metabolic disorders than skipping breakfast [11,14]. Conversely, other studies observed dinner skipping as a significant predictor of weight gain and obesity [13,25]. Again, other studies report that skipping dinner results in a higher total energy expenditure than skipping breakfast. Diet-induced thermogenesis was lower in the evening and at night than in the morning. Eating the same meal in the evening instead of the morning leads to a decrease in metabolic rate and triggers higher glycemic responses due to variations in energy expenditure and metabolic processes that occur as part of our circadian rhythm [26]. Thus, the results of our study contribute to the growing body of evidence that skipping dinner has a protective effect compared to skipping breakfast and skipping lunch because it is only associated with higher HDL-C levels but with no other cardiometabolic risk factors.
However, the limitations of this study should be considered when interpreting the results. One major limitation of this study is its cross-sectional design, which prevented the establishment of causal relationships between the types of meal skipping and the development of the cardiometabolic risk factors. Recall bias could exist, as dietary data were collected through self-report surveys. Although our study adjusted for confounding factors, such as sociodemographic and lifestyle factors, preexisting cardiometabolic diseases, age, and sex, it is advised to consider that meal skipping patterns could also be influenced by these factors as well as other unexamined variables. For example, the difference between various occupations due to differences in working hours and working environment also influencing eating habits and lifestyle must be considered; thus, further investigations stratified by occupation may be required.
Despite these limitations, our study has several strengths and contributes important findings. First, our study is the first to investigate the association between cardiometabolic risk factors and eight mutually exclusive and collectively exhaustive meal-skipping habits. Second, our study involved a large nationwide population-based sample that enabled us to examine all frequency patterns of meal skipping, particularly lunch and dinner skipping. Third, our analyses were not only elaborately adjusted for basic potential confounding variables such as sociodemographic and lifestyle factors, BMI, total energy intake, and preexisting diseases, but were also individually adjusted for the intake of medications related to individual cardiometabolic risk factors. Moreover, our statistical analyses were conducted in two versions of the sample to confirm the robustness of our results: first, with all participants and second, with only healthy participants.
Overall, our findings strongly suggest a significant association between irregular breakfast consumption and cardiometabolic risk factors, and a less strong but still significant correlation between irregular lunch consumption and cardiometabolic risk factors. Although the small increase in biomarkers associated with skipping breakfast and/or lunch may seem relatively modest, its potential impact on public health is considerable because of the widespread prevalence of skipping breakfast, which exceeds 30% in Korea. A pooled analysis of 1.4 million participants worldwide demonstrated that a 1 mmol/L increase in total cholesterol was associated with 44% and 20% higher risks of IHD and ischemic stroke, respectively [27]. Therefore, promoting the dietary habit of regular breakfast consumption and, if possible, regular lunch consumption could play a crucial role in preventing metabolic disorders. Based on this study, we suggest that skipping dinner, rather than breakfast or lunch, is more beneficial in terms of cardiovascular and metabolic risk factors. Thus, it would be recommended for Korean adults wishing to cut down on one meal instead of having all three regular meals for various personal reasons to not skip breakfast but dinner.
In conclusion, this study showed that for South Korean adults, breakfast skipping, and lunch skipping to a lesser degree, was significantly associated with increasing cardio-metabolic risk factors compared to regular meal consumers. However, skipping dinner showed no significant association with the cardiometabolic risk factors. Therefore, our study suggests that regular breakfast and lunch consumption may be important in preventing and managing cardiometabolic disorders. Considering the current changing dietary habits and trends in regular meal consumption per day, the dietary behavioral guideline we provide for promoting cardiometabolic health is to skip dinner rather than breakfast.